- Available
- XML
- Multimedia
- Download citation
- Statistics
- Share




Acceptability of COVID-19 vaccination in Herat, Afghanistan
 1,2, Ahmad Neyazi 3,Attaullah Ahmadi 4, Omid Tabesh5, Habibah Afzali 6✉, Kenesh Dzhusupov7, Md Shariful Islam8, Rayan Rachmad Nugraha9, Blaise Ntacyabukura10, Shyam Sundar Budhathoki11Lin Xu12, Wahid Majrooh13
1,2, Ahmad Neyazi 3,Attaullah Ahmadi 4, Omid Tabesh5, Habibah Afzali 6✉, Kenesh Dzhusupov7, Md Shariful Islam8, Rayan Rachmad Nugraha9, Blaise Ntacyabukura10, Shyam Sundar Budhathoki11Lin Xu12, Wahid Majrooh13show more
| Received 07 June 2021 |
Accepted 28 Oct 2021 |
Published 24 Nov 2021 |
Abstract
Background: COVID-19 vaccine hesitancy is one of the major concerns in the roll out of vaccines in many countries. The aim of the study was to assess the level of COVID-19 vaccine acceptability among the population in Herat, Afghanistan, the third largest city in the country.
Methods: This cross-sectional study was conducted between 15 April 2021 and 20 April 2021 among the general population of Herat City to examine the acceptability rate of COVID-19 vaccine. Sample size was calculated at 555. Different variables were collected using a questionnaire developed. Data were evaluated in IBM SPSS program.
Results: Only 10.63% of the participants were willing to receive COVID-19 vaccine without having any concern and reservation. 45% were willing to receive the COVID-19 vaccine. 66.5% were concerned about the vaccine and its side effects and 29% were afraid of being infected by transmission of COVID-19 through the administration of vaccine on them.
Conclusion: This research demonstrates that, concerns about the vaccine, myths and misinformation are widespread which will undermine the vaccination process. This study recommends the initiation of more health-related campaigns and awareness programs by the government for general population to enhance and expedite the roll out of COVID-19 vaccine.
Keywords: Concerns, Acceptancy, Vaccine hesitancy, Vaccination, COVID-19, Herat-Afghanistan.
1. Introduction
In December 2019 a novel coronavirus called Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) which causes an illness called Coronavirus Disease 2019 (COVID-19) was discovered in Wuhan City of Hubei Province of China (1). The disease was declared a pandemic by the World Health Organization (WHO) on 11 February 2020 after it was announced a Public Health Emergency of International Concern (PHEIC) on January 2020 (2, 3). Aside from the impact of COVID-19 on health, its implication on economic situation is undeniable. It has resulted in a significant rise in unemployment rate globally (4).
There are three most common symptoms in patients with COVID-19, which appear differently for different people. Fever, dry cough, and tiredness are the most common symptoms of COVID-19. Symptoms may appear 2-14 days after exposure to the virus (5). Extra pulmonary symptoms are also common in some patients; for example, loss of sense of smell, cardiac involvement, acute kidney injury, coagulation disorders, and thrombotic complications could be associated with poor prognosis (6-7).
As the number of infected people with COVID-19 keeps growing globally, many of the pharmaceutical companies started to develop a vaccine to prevent the COVID-19 infection (8). The speed for developing the vaccine to end this pandemic has been accelerated surprisingly fast (9). Several vaccines have been approved to be used in many countries (9). The first mass vaccination program for COVID-19 started in December 2020 (10). According to the WHO, by 9 March 2021, more than 268 million doses of COVID-19 vaccines have been administered globally (11). The vaccine’s very common side effects are joint pain, headache, nausea, chills, and fatigue, generally feeling unwell, warmth, pain and tenderness. Its common side effects are swelling in injection point, fever, vomiting or diarrhea, pain in legs or arms, runny nose, cough and chills. The side effects may occur in 6 to 8 hours after vaccination and may last for 2 to 3 days (14). For decades, vaccination has been playing a key role in preventing deadly diseases (15).
COVID-19 vaccination program in Afghanistan started on 23 February 2021 using the vaccines donated by India (12). Currently in Afghanistan, the SII-AstraZeneca also known as COVISHIELD (licensed and manufactured by Serum Institute of India) vaccine by Coalition for Epidemic Preparedness Innovations (CEPI), Global Alliance for Vaccines and Immunization (GAVI), and the WHO are being administered. In the first shipment via the COVAX facility to Afghanistan in 8 March 2021, 468,000 doses of COVID-19 vaccine were included (13). Afghanistan was the first country in Central Asia to receive the vaccine through COVAX (15).
Vaccine hesitancy is a significant concern globally and Afghanistan is not spared (16). In Afghanistan misinformation, rumors and believes about vaccine and vaccination is a major problem that decreases the acceptance level of vaccination by general population (17). Vaccine hesitancy remains a formidable challenge against eradication of fatal diseases such as polio in Afghanistan, making the country one of the two remaining countries endemic for polio (18).
This study aims to evaluate acceptability rate of COVID-19 vaccine among Herat – Afghanistan population during the vaccination and to find out the reasons behind COVID-19 vaccination hesitancy.
2. Materials and Methods
Study design, place, and duration
This cross-sectional study was conducted on 15 April 2021 to 20 April 2021 among population of Herat city of Afghanistan.
Sample size
Sample size was calculated using the sample calculation approach for prevalence studies. As there is no prior study on evaluation of COVID-19 vaccine acceptability rate among population of Afghanistan, in this method, acceptability was taken as 0.50, d was taken as 0.05 and z was taken as 1.96. The minimum sample size was calculated as 384 but we collected 555 people data.
Data collection
Each participant filled a questionnaire containing 28 questions. The socio-demographic sub-scale contained 7 questions. The knowledge and perspective sub-scale contained 6 questions and the attitude sub-scale contained 15 questions. The data collection was done by medical students from Herat city. Prior to the start of data collection, the data collectors were trained for 4 hours in two days so that they can interact with volunteers and demonstrate the study goal and take a consent letter from the participants. Data was collected from all the 15 districts of Herat city and the questionnaire was distributed randomly to people who were willing to participate regarding the inclusion and exclusion criteria.
Inclusion and exclusion criteria
Participants in this study were aged above 18 years old male and female residents of Herat city of Afghanistan who voluntarily participated in this research project. Non-volunteer and health workers were excluded from this research.
Study Scale and Statistical Analysis
The questionnaire was developed based on literature review in Dari language. The two official languages that people use to communicate in their daily lives are Pashto and Dari (19). A pilot study was conducted among 20 male and female participants; no major changes were required.
The final Dari version of the questionnaire consisted of three parts. The first section was designed to collect the participants’ socio-demographic information including participants’ age, gender, marital status, educational level, economic status, occupation, and presence of any chronic diseases. The age variable had six categories: 18-24 years old, 25-34 years old, 35-44 years old, 45-54 years old, 55-64 years old, and higher than 65 years old. Gender variable was divided into two categories: Male and Female. Marital status variable had four categories: Single, Married, Widow, and Divorced. Educational level variable had five categories: Illiterate, Primary school, Secondary school, High school, and University. Economic status variable had three categories: High income, Medium income, and Low income. Occupation variables had six categories: Permanent, Owner, Contract, Unemployed, Retired, and Other. The presence of chronic disease variable had two categories: “Yes”, and “No”. The second section was designed to collect the participants’ general information and perception about COVID-19. The “Taken influenza vaccine?” variable had two categories: “Yes”, and “No”. The “Cure for COVID-19 exists” and “Do you think you have been infected with SARS-CoV-2” variables had three categories each: “Yes”, “No”, and “Don’t know”. The “To what extent do you think coronavirus poses a risk to you personally?” variable had six categories: “Major risk”, “Significant risk”, “Moderate risk”, “Minor risk”, “No risk at all”, and “Don’t know”. The “Which COVID-19 vaccine is better to use?” variable had four categories: “Pfizer-BioNTech”, “Johnson & Johnson’s Janssen”, “AstraZeneca”, and “Don’t know”. The “Will you vaccinate against COVID-19” variable had two categories: “Yes”, and “No”. The third section was designed to collect the participants’ attitude and practice towards COVID-19 vaccine acceptability. This section contained 15 questions covering all the possible concerns about the participants’ attitude towards COVID-19 vaccination. All the variables in the third section had two categories: “Yes”, and “No”. All the variables values were added based on a series, in left to right and top to bottom order in IBM SPSS software starting from 1.
The participants were divided into two groups. The ones who were willing to be vaccinated and the ones who were not, based on their answers on the third section and their socio-demographic characteristics. At the end, it resulted in three major categories of participants. The first category consisted of the participants who were willing to vaccinate themselves without any concern. The second category consisted of the participants who were willing to vaccinate themselves despite having their concerns, and the third category consisted of the participants who were not willing to vaccinate themselves with or without having any concerns.
Dataset was evaluated by IBM SPSS software version 25.0. Categorical variables were presented with numbers (n) and percentage (%) and Chi-square test was used to observe the difference between categorical variables.
Ethical approval
Ethical approval was obtained from the AMSA Medical Research Center Ethical Committee on 10th April 2021.
3. Results
Five hundred fifty-five participants were enrolled in this study. 73.3% of the participants aged between 18-44 years old. In this study, 51.5% were females, 37.1% single, 28.7% illiterate, 83.6% with an average economic status and 1.6% with a chronic disease. (Table 1)

4.7% of the participants had taken the influenza vaccine, 37.3% of the participants believed that there is a cure for COVID-19, 42.0% of the participants replied “No” to the question if they were infected with COVID-19, 27.9% of the participants replied that the coronavirus poses a “Moderate risk” to their health, 95.9% of the participants were not aware of the vaccines or even the vaccines’ names and 45.0% of the participants were willing to vaccinate themselves if the vaccine becomes available for them. (Table 2)

37.8% (210) of the participants were concerned about the vaccine efficacy, 66.5% (369) of the participants expressed that they are concerned about the COVID-19 vaccine and its side effects. 29.0% of the participants were worried about the virus transmission to them through vaccine. 10.6% of the participants replied that they do not want to be the first to get the vaccine as it is new. 3.6% of the participants believed that the vaccine causes autism. 11.0% of the participants replied that the COVID-19 vaccine affects the fertility. Only 11.7% (65) of the participants replied that they do not have any concern about the COVID-19 vaccine. (Table 3)

Association of the participants’ educational level with willingness to vaccinate considering their concerns about COVID-19 vaccines are presented in Table 4. Of all the participants 9 illiterate, 13 with primary school educational level, 3 with secondary school educational level, 19 with high school educational level, and 15 with university educational level accepted to vaccinate themselves if the vaccine becomes available, without having any concern. 41 illiterate participants, 41 participants with primary school educational level, 40 participants with secondary school educational level, 42 participants with high school educational level, and 27 participants with university educational level were willing to vaccinate themselves despite having their concerns regarding the vaccine and vaccination. (Table 4)

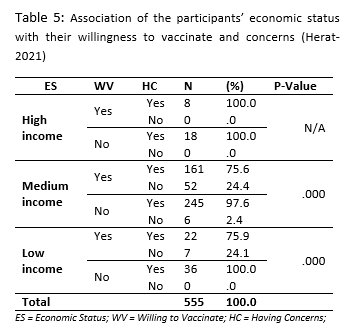
Association of the participant’s economic status with their willingness to vaccinate considering their concerns are presented in Table 5. All of the participants with high income and willing to vaccinate themselves had their concerns about the vaccine and vaccination. 161 participants with medium income, and 22 with low income who were willing to vaccinate themselves had their concerns regarding the vaccine. 52 participants with medium income and 7 participants with low income were willing to vaccinate themselves without having any concerns regarding the vaccine. (Table 5)
4. Discussion
We conducted this research to assess COVID-19 vaccine acceptability rate among the population of Herat, Afghanistan who were selected randomly. 45% of the participants responded that they will vaccinate themselves with or without having concerns about the vaccine. 10.6% of the participants were willing to vaccinate themselves without any worries about the side effects and the vaccine’s effectiveness. 34.4% of the participants responded that they will vaccinate themselves despite having concerns about COVID-19 vaccine’s effectiveness or its side effects.
A global survey in 19 countries with a high COVID-19 burden published in Nature Medicine shows that 71.5% of the participants are willing to vaccinate themselves (20). Another study published in Vaccines shows that 62.1% of adults in Japan are willing to vaccinate themselves if one become available (21). Vaccine hesitancy is common but compared to previous studies (20-22, 24-28), participants of this study were more concerned and hesitant about the COVID-19 vaccine. The main reasons are the people’s low level of education, myths and false information spreading around about COVID-19 and its vaccine in Herat city.
As shown in Table 3, incredulity in vaccine efficacy is one of the major concerns of the participants which influences the COVID-19 vaccine acceptability. The belief in vaccine efficacy is directly proportional to high vaccine acceptability rate. A study in Indonesia, shows that 93.3% of the participants accept to vaccinate using a vaccine with 95% of effectiveness while 67.0% of the participants accepted to vaccinate themselves using a vaccine with 50% of effectiveness (23).
In terms of hesitancy of vaccine, our study result is in line with previous vaccination campaign reports for polio and other vaccines as the UNICEF reports that vaccine hesitancy due to spread of rumors and misinformation is growing (17). Our finding shows that only 45.0% of participants are willing to vaccinate themselves against COVID-19 and 55% of them were not willing to take vaccine against COVID-19.
We found a significant association between educational level and economic status and COVID-19 vaccine acceptancy. There was no significant association between the participants who have taken the Influenza vaccine and the ones who were willing to take COVID-19 vaccine. This variation could be due to low awareness campaigns on COVID-19 vaccination program by government and other organizations working in health sector and mass COVID-19 vaccine myths among people living in Herat city which caused people to have less information on COVID-19 vaccine.
Stress and fear due to the COVID-19 disease among people can have its impact on the level of COVID-19 vaccine acceptancy. A survey conducted among general population of Herat province of Afghanistan shows that at the early days of the pandemic in Herat province of Afghanistan, 52.5% of the people were feeling depressed, worried or anxious while 53.9% of them were using mask to protect themselves against COVID-19 (29). Another study conducted a few months after starting of the COVID-19 in Afghanistan, published in Razi International Medical Journal shows that peoples’ observance of quarantine and social distancing protocols waned compared to the early days of the pandemic (30). In this study, only 18.8% of the participants were thinking of the COVID-19 as a major risk to them. This shows that people’s willingness to vaccinate themselves against COVID-19 may rise with increasing the level of people’s fear due to COVID-19.
Although COVID-19 vaccination coverage in Afghanistan is not as high as other countries, vaccination inequalities are the issues that should be prioritized to address. Lots of studies show that vaccine inequalities are major concerns even in developed countries (31-38).
5. Limitation of the study
The limitation of this study is that it did not cover the districts of Herat due to the security issues. The data was not collected from each part of Herat city equally. Another limitation of the study is that it does not imply causality.
6. Conclusion
This study provides insights into COVID-19 vaccine acceptability among the population of Herat, Afghanistan. Results show that less than half of the city’s population are willing to get themselves vaccinated despite having concerns about the vaccine. Concerns about the vaccine, myths and misinformation are widespread which worsen the vaccination process. This study presents the need for more health-related campaigns and awareness programs for general population to boost and expedite the roll out of COVID-19 vaccine.
7. Author contributions
All authors made substantial contribution to conception and design, data collection and data entry, data analysis and their interpretation, drafting the article and giving the final approval of the version to be published, and agreed to be accountable for all aspects of work.
8. Consent for publication
A detailed description of the study, benefits, confidentiality was explained during the initial contact with the participants prior to their participation. A written consent letter was obtained from all the participants involved in this research.
9. Conflict of interest
The authors declare no conflict of interest.
10. Funding
This research received no external funding.
10. Acknowledgement
We would like to express our sincere gratitude to all the participants who enrolled in this study.
11. References
- Wu F, Zhao S, Yu B, Chen YM, Wang W, Song ZG, Hu Y, Tao ZW, Tian JH, Pei YY, Yuan ML. A new coronavirus associated with human respiratory disease in China. Nature. 2020 Mar;579(7798):265-9.
- Tengilimoğlu D, Zekioğlu A, Tosun N, Işık O, Tengilimoğlu O. Impacts of COVID-19 pandemic period on depression, anxiety and stress levels of the healthcare employees in Turkey. Legal Medicine (Tokyo, Japan). 2021 Feb;48:101811.
- Al-Hanawi MK, Angawi K, Alshareef N, Qattan AM, Helmy HZ, Abudawood Y, Alqurashi M, Kattan WM, Kadasah NA, Chirwa GC, Alsharqi O. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Frontiers in Public Health. 2020;8.
- Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, Agha M, Agha R. The socio-economic implications of the coronavirus and COVID-19 pandemic: a review. International journal of surgery. 2020 Apr 17.
- Coronavirus Disease 2019 (COVID-19) – Symptoms [Internet]. Centers for Disease Control and Prevention. 2021 [cited 3 June 2021]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html
- Lai CC, Ko WC, Lee PI, Jean SS, Hsueh PR. Extra-respiratory manifestations of COVID-19. International journal of antimicrobial agents. 2020 Aug 1;56(2):106024.
- Miller R, Englund K. Clinical presentation and course of COVID-19. Cleveland Clinic journal of medicine. 2020 May 5.
- Different COVID-19 Vaccines [Internet]. Centers for Disease Control and Prevention. 2021 [cited 1 May 2021]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines.html
- O’Callaghan KP, Blatz AM, Offit PA. Developing a SARS-CoV-2 vaccine at warp speed. Jama. 2020 Aug 4.
- Coronavirus disease (COVID-19): Vaccines [Internet]. Who.int. 2021 [cited 1 May 2021]. Available from: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-vaccines
- WHO news updates [Internet]. Who.int. 2021 [cited 1 May 2021]. Available from: https://www.who.int/news-room/news-updates
- واکسیناسیون کرونا در افغانستان آغاز شد - BBC News فارسی [Internet]. BBC News فارسی. 2021 [cited 1 May 2021]. Available from: https://www.bbc.com/persian/afghanistan-56165443
- COVAX roll-out – Afghanistan [Internet]. Gavi.org. 2021 [cited 6 May 2021]. Available from: https://www.gavi.org/covax-vaccine-roll-out/afghanistan
- COVISHIELD FAQs - Serum Institute Of India. [Internet]. Seruminstitute.com. 2021 [cited 2 June 2021]. Available from: https://seruminstitute.com/health_faq_covishield.php
- WHO | Vaccination greatly reduces disease, disability, death and inequity worldwide [Internet]. Who.int. 2021 [cited 1 May 2021]. Available from: https://www.who.int/bulletin/volumes/86/2/07-040089/en/
- Geoghegan S, O’Callaghan KP, Offit PA. Vaccine safety: myths and misinformation. Frontiers in microbiology. 2020 Mar 17;11:372.
- Polio eradication [Internet]. Unicef.org. 2021 [cited 1 May 2021]. Available from: https://www.unicef.org/afghanistan/polio-eradication
- Ahmadi A, Essar MY, Lin X, Adebisi YA, Lucero-Prisno III DE. Polio in Afghanistan: the current situation amid COVID-19. The American Journal of Tropical Medicine and Hygiene. 2020 Oct 7;103(4):1367-9. DOI: https://doi.org/10.4269/ajtmh.20-1010.
- Herat - English [Internet]. English. 2021 [cited 1 May 2021]. Available from: https://president.gov.af/en/herat/
- Lazarus JV, Ratzan SC, Palayew A, Gostin LO, Larson HJ, Rabin K, Kimball S, El-Mohandes A. A global survey of potential acceptance of a COVID-19 vaccine. Nature medicine. 2021 Feb;27(2):225-8.
- Machida M, Nakamura I, Kojima T, Saito R, Nakaya T, Hanibuchi T, Takamiya T, Odagiri Y, Fukushima N, Kikuchi H, Amagasa S. Acceptance of a COVID-19 Vaccine in Japan during the COVID-19 Pandemic. Vaccines. 2021 Mar;9(3):210.
- Wang J, Jing R, Lai X, Zhang H, Lyu Y, Knoll MD, Fang H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines. 2020 Sep;8(3):482.
- Harapan H, Wagner AL, Yufika A, Winardi W, Anwar S, Gan AK, Setiawan AM, Rajamoorthy Y, Sofyan H, Mudatsir M. Acceptance of a COVID-19 vaccine in southeast Asia: A cross-sectional study in Indonesia. Frontiers in public health. 2020;8.
- Murphy J, Vallières F, Bentall RP, Shevlin M, McBride O, Hartman TK, McKay R, Bennett K, Mason L, Gibson-Miller J, Levita L. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nature communications. 2021 Jan 4;12(1):1-5.
- Yoda T, Katsuyama H. Willingness to Receive COVID-19 Vaccination in Japan. Vaccines. 2021 Jan;9(1):48.
- Williams L, Flowers P, McLeod J, Young D, Rollins L. The CATALYST Project Team. Social Patterning and Stability of Intention to Accept a COVID-19 Vaccine in Scotland: Will Those Most at Risk Accept a Vaccine. Vaccines 2021, 9, 17.
- Fisher KA, Bloomstone SJ, Walder J, Crawford S, Fouayzi H, Mazor KM. Attitudes toward a potential SARS-CoV-2 vaccine: a survey of US adults. Annals of internal medicine. 2020 Dec 15;173(12):964-73.
- Neumann-Böhme S, Varghese NE, Sabat I, Barros PP, Brouwer W, van Exel J, Schreyögg J, Stargardt T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19.
- SHAYAN N, NEYAZI A, AFZALI H, KONŞUK ÜNLÜ H, ÖZCEBE H. Survey on Community Awareness and Risk Perception on COVID-19 in Herat. Sağlık ve Toplum [Internet]. 2021 [cited 2 June 2021];21(1):60-68. Available from: https://ssyv.org.tr/wp-content/uploads/2021/04/7-Heratda-COVID-19-Hakkinda-Toplum-Bilinci-ve-Risk-Algilamasi-Uzerine-Bir-Arastirma.pdf
- Shayan NA, Azizi AT, Razaqi N, Afzali H, Neyazi A, Waez H, Noormohmmadi M, Bhattacharya S. Phase wise assessment of COVID-19 related depression, anxiety, and stress level among patients in Herat city, Afghanistan-A descriptive study. Razi International Medical Journal. 2021 May 24;1(1).
- Marlow LA, Wardle J, Forster AS, Waller J. Ethnic differences in human papillomavirus awareness and vaccine acceptability. J Epidemiol Community Health. 2009 Dec 1;63(12):1010-5.
- Loiacono MM, Mahmud SM, Chit A, van Aalst R, Kwong JC, Mitsakakis N, Skinner L, Thommes E, Bricout H, Grootendorst P. Patient and practice level factors associated with seasonal influenza vaccine uptake among at-risk adults in England, 2011 to 2016: An age-stratified retrospective cohort study. Vaccine: X. 2020 Apr 9;4:100054.
- Tiley KS, White JM, Andrews N, Ramsay M, Edelstein M. Inequalities in childhood vaccination timing and completion in London. Vaccine. 2018 Oct 29;36(45):6726-35.
- Wagner KS, van Wijgerden JC, Andrews N, Goulden K, White JM. Childhood vaccination coverage by ethnicity within London between 2006/2007 and 2010/2011. Archives of disease in childhood. 2014 Apr 1;99(4):348-53.
- Campos-Matos I, Mandal S, Yates J, Ramsay M, Wilson J, Lim WS. Maximising benefit, reducing inequalities and ensuring deliverability: Prioritisation of COVID-19 vaccination in the UK. The Lancet Regional Health-Europe. 2021 Mar 1;2.
- Gupta R, Morain SR. Ethical allocation of future COVID-19 vaccines. Journal of medical ethics. 2021 Mar 1;47(3):137-41.
- Burgess RA, Osborne RH, Yongabi KA, Greenhalgh T, Gurdasani D, Kang G, Falade AG, Odone A, Busse R, Martin-Moreno JM, Reicher S. The COVID-19 vaccines rush: participatory community engagement matters more than ever. The Lancet. 2021 Jan 2;397(10268):8-10.
- Cheong MW, Allotey P, Reidpath DD. Unequal Access to Vaccines Will Exacerbate Other Inequalities. Asia Pacific Journal of Public Health. 2020 Sep;32(6-7):379-80.