- Available
- XML
- Download citation
- Statistics
- Share




Validity and reliability of the Dari version of the CES-D scale among the general population of Herat, Afghanistan: A methodological study
 1✉, Nurperihan Tosun 2, Farooq Hosaini3, Surasak Saokaew 4
1✉, Nurperihan Tosun 2, Farooq Hosaini3, Surasak Saokaew 4show more
| Received 06 Nov 2021 |
Accepted 02 Mar 2022 |
Published 25 May 2022 |
Abstract
Background: Depression is considered one of the significant pressing public health problems globally. The Center for Epidemiologic Studies Depression (CES-D) scale is valuable for assessing subthreshold depression. The purpose of this study was to investigate various aspects of the CES-D scale's validity and reliability in the Afghan population.
Methods: This methodological study was conducted between 6th June 2021 and 12th July 2021 among the general population in the Herat province of Afghanistan. A total of 424 participants filled out the questionnaires provided to them. The forward-backward translation method translated the CES-D scale into the Dari language. The data was statistically analyzed using IBM SPSS version 24.0 and AMOS version 24.0 software for Windows. Exploratory (EFA) and confirmatory factor analysis were used to assess the factor structure (CFA). The reliability was assessed by Cronbach’s alpha, inter-item correlation, and total item correlation.
Results: The exploratory factor analysis resulted in three factors (Depressed affect & Somatic complaints factor, the Interpersonal factor, and the Positive affect factor). The CFA result suggested that the resulted model of the Dari version of the CES-D scale with 19 items was the best fit for our data. The Cronbach’s alpha for the 19 items scale was 0.874.
Conclusion: The results of this study show that the Dari version of the CES-D scale is valid and reliable to use among the general population of Herat province of Afghanistan. The scale can assess depression and its symptoms among the population mentioned above with confidence.
Keywords: CES-D Scale, Depression, Validity, Reliability, Cultural Adaptation, Herat-Afghanistan.
1. Introduction
Depression is considered one of the world's most significant public health issues. According to the World Health Organization (WHO), more than 300 million people, or about 4.4% of the world's population, suffer from depression (1). Sadness, disinterest or joylessness, feelings of guilt or low self-esteem, sleep or eating disorders, fatigue, and poor concentration are symptoms of depressive disorders. Depression can be chronic or recurrent and severely limit a person's ability to function at work or school or manage daily life (1-2). It has also been described as a comorbidity for other diseases because it is associated with mortality and poor health (3-6). According to WHO (World Health Organization), depression or depressive disorders can be divided into two main categories: Major Depression/Depressive Episode and Dysthymia (7-8).
Four depression scales and databases which are most commonly used are the Center for Epidemiological Studies Depression Scale (CES-D), the Beck Depression Inventory (BDI), the Hamilton Rating Scale for Depression (HRSD), and the Zung Self-Rating Depression Scale (SDS). The BDI, the CES-D, the HRSD, and the SDS can all capture a single, overarching, and general depression factor and various lower-level specific depression symptom components. The CES-D is considered the most useful scale to assess depression (9-14). It is a self-report scale developed based on other depression assessments to assess symptoms of depression in the general population. The CES-D scale was developed in 1970. It was created to be used in epidemiologic research to determine the severity of depressive symptoms and to identify those who are at risk of developing depression in the general population (8). The CES-D scale contains 20 items, each of which has a specific role in assessing relevant symptoms of depression (8, 14-15). However, despite the widespread use of the CES-D, its latent structure has been questioned (16-17).
The CES-D scale is often used in epidemiological studies. However, it is usable for epidemiological studies and clinical practice (8). In Afghanistan, where there are large numbers of unemployed people, daily attacks by terrorists throughout the country affect people's mental health (18-20).
The purpose of this study was to investigate various aspects of the CES-D scale's validity and reliability in the Afghan population.
2. Materials and Methods
CES-D
CES-D scale is a 20-item questionnaire developed to measure depression-related symptoms. The original CES-D scale has four factors. The Depressed affect factor consists of seven items (CES-D 3, CES-D 6, CES-D 9, CES-D 10, CES-D 14, CES-D 17, CES-D 18). The Positive affect factor consists of four items (CES-D 4, CES-D 8, CES-D 12, CES-D 16). The Somatic complaints factor consist of seven items (CES-D 1, CES-D 2, CES-D 5, CES-D 7, CES-D 11, CES-D 13, CES-D 20). The fourth factor is the Interpersonal factor, consisting of two items (CES-D 15, CES-D 19) (34). Each item of the CES-D scale has four options from 0 to 3 and responds from low to the high occurrence of the symptom. The result of the total of 20 items scale results in a 0 to 60 score. A result of lower than 16 is indicative of normal (mild depressive symptomatology). Depression is indicated by a total score of 16 or higher. Each item of the CES-D scale measures the magnitude of depression (35).
Translation of CES-D
The translation and cultural adaptation of the Dari version of the CES-D scale was made in three steps, using the forward-backward translation method to achieve this goal. First, three independent psychologists translated the CES-D scale into the Dari language. Second, the translated version was reviewed by three individuals and a Dari literature professor to check its readability, comprehensibility, Afghan culture, and appropriateness. The changes suggested by the reviewers were implemented. Third, the English specialist back-translated the resulting questionnaire into English. The back-translated English questionnaire was compared to the original English CES-D scale. The outcomes were almost identical. Minor differences in word and sentence structure were noted, but the meaning of the sentences was the same. No changes were required. The version of the CES-D scale translated into Dari was used for a pilot study with 30 people. They reported no difficulty in reading and understanding the items of the questionnaire. The result of the pilot study was analyzed and interpreted by the team, and a final version of the questionnaire was prepared after the minor necessary changes were made to the translated scale. The final questionnaire used for this study included two parts. The first part of the questionnaire had 11 items to collect the participants' socio-demographic data. The second section of the questionnaire used in this study contained the CES-D scale's items.
Data collection
The data collection of this study was done between 6th June 2021 and 12th July 2021. This Dari version of the CES-D scale was administered among the general population of Herat province aged above eight years old. The sample size was determined using the CES-D scale's number of items. For each item, 20 participants were taken. Therefore, for 20 items of the CES-D scale, 400 participants were needed plus almost 5% to cover the error. Therefore, 424 participants participated in this study.
Statistical Analysis
The collected data was entered into IBM Statistical Package for the Social Sciences (SPSS) version 24.0 software for windows, and the statistical analyses were performed on this software as well as AMOS (Version 24.0). The socio-demographic characteristics of the participants were evaluated and presented by numbers (N) and percentages (%). Items of the scale were represented and evaluated using the Descriptive method and presented by Mean and SD (Standard Deviation). The factor structure was determined using exploratory factor analysis using the principal component analysis with Varimax rotation. Items of factors loaded with a score greater than 0.3 in the Communalities table were considered significant (considering the sample size). The Kaiser-Meyer-Olkin statistic and Bartlett's test were used for factor analysis to evaluate the internal consistency of the items, and Cronbach's alpha coefficients were used. The values of Cronbach's alpha of more than 0.6 were considered satisfactory.
Confirmatory factor analysis was used to determine the goodness-of-fit of the Dari version of the CES-D scale. The following parameters were used to achieve this goal: “Chi-Square to df ratio” (CMIN/df), which was considered permissible, the resulted value was less than 5. The “Comparative Fit Index” (CFI) was considered >0.8 as permissible. The “Goodness-of-Fit Index” (GFI) was considered the resulting value of >0.95 as permissible. The “Adjusted Goodness-of-Fit Index” considered the resulting value of >0.80 as permissible. The “Tucker-Lewis Index” (TLI) was considered the value of >0.95 as permissible. The “Standardized Root Mean Square Residual” (SRMR) was considered the value of <0.9 as acceptable. The “Root Mean Square Error of Approximation” (RMSEA) was considered the value between 0.05 – 0.10 as moderate and acceptable (36).
In addition, to the scale's reliability, the Guttman split-half Coefficient and the Spearman-Brown Correlation Coefficient were used. The test-retest reliability result above 0.6 was considered satisfactory. Based on the study's sample size, a p-value of less than 0.05 was considered the indicator of statistical significance for results in this study.
3. Results
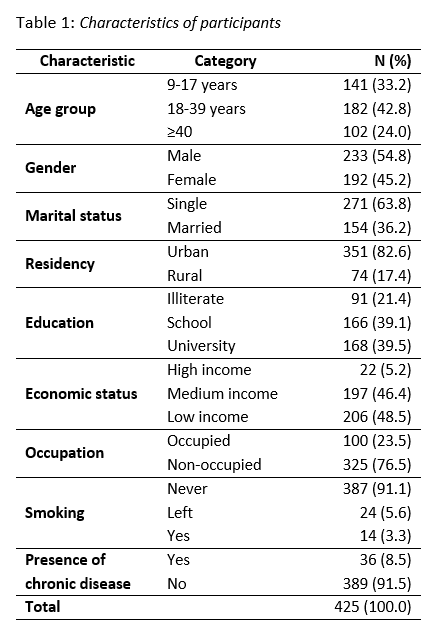
Four hundred twenty-five participants were interviewed in this study. 33.2% of the participants were aged between 9 and 17 years old. 42.8% of the participants were aged between 18 and 39 years old. 54.8% of the participants were male, 82.6% lived in urban areas of Herat province, 21.4% were illiterate, 46.4% had an average economic status, and 8.5% had a chronic disease. (Table 1)
The items of the original CES-D scale are presented by items’ Mean and Standard Deviation values. (Table 2)

The explanatory factor analysis yielded a three-factor solution with a large eigenvalue of 6.388 for the first factor followed by two factors with an eigenvalue larger than 1. The first factor comprised 13 items that expressed the depressed mode. The second factor is comprised of two items related to and expressed the interpersonal relationship. The third factor that comprised four items expressed positive feelings. Also, the explanatory factor analysis resulted in a two-factor solution by fixing the number of factors to extract to two. The 2F-1 with an eigenvalue of 6.388 comperes 15 items that expressed feelings, behavior, and thoughts related to depressed mode. And the 2F-2 with an eigenvalue of 1.935 comprised of r items that expressed positive feelings. The reliability of the CES-D scale was examined using Cronbach’s alpha which was found to be high at 0.824. The Split-half coefficients were also found to be high at 0.720. (Table 3)

The factor analysis using Cronbach’s Alpha resulted in the total item correlation being high enough, ranging from 0.430 to 0.725. But it also resulted to some low values of 0.077, 0.185, 0.290, 0.320, 0.364, and 0.363 for items 4 (as good as others), 7 (too much effort), 8 (hopeful), 12 (happy), 15 (unfriendly people), 16 (enjoy life), and 19 (other dislike me). However, the investigation of the internal consistencies of the three extracted factors’ correlation resulted as follows: The correlation of four items related to the positive feelings factor was found to be high enough, ranging from 0.432 to 0.532 except for item 4 (as good as others) which was found 0.272; The correlation of the two items related to interpersonal factor was found to be high enough; The correlation of the 14 items related to negative feelings factor was found to be high enough ranging from 0.446 to 0.738 with a quite high Cronbach’s alpha except for the item 7 (too much effort) which was found to be 0.272. (Table 4)

As shown in Table 4, item 7 of the CES-D scale did not result in the minimum needed Cronbach’s alpha. In the validation process of the Dari version of the CES-D scale in the Herat province of Afghanistan, this item has been deleted. (Table 5)

The confirmatory model for the CES-D scale resulted in the following components: CMIN/df was found at 4.363; CFI was found at 0.833; GFI was found at 0.868; AGFI was found at 0.832; TLI was found at 0.808; SRMR was found 0.000; RMSEA was found 0.089. (Figure 1)

4. Discussion
While self-administered scales save time for data collectors and researchers, they are highly dependent on the reading ability and cooperation of the study participants. On the other hand, there are not enough reliable and valid studies conducted, nor do enough different translations of the scale exist. This is also applicable to the Zung Depression Rating Scale (21-23). We conducted this study to assess the reliability and validity of the Dari version of the CES-D scale among the general population of Herat province of Afghanistan who was selected randomly. This study demonstrates that the Dari version of the CES-D scale's internal consistency and test-retest reliability is high. Confirmatory factor analysis revealed that the scale's normed fit index value was less than the optimal value. After one of the scale's items was removed (Item 7), Cronbach's alpha for the total items was found to be 0.874. The factor analysis showed three factors that explain the "Positive feelings factor", "Negative feelings factor," and "Interpersonal relationship factor." In a meta-analysis study of the factor structures of the CES-D, it was found that the scale generally has a 3-factor structure (37).
The literature contains studies on the validity and reliability of the scale in different languages and populations. The Greek study had a Cronbach's alpha of 0.95, and factor analysis showed that three factors explained 66% of the total variance of the CES-D: "positive affect," "irritability and interpersonal relations," and "depressed affect and somatic complaints." Therefore, the Greek study is reliable, valid, and suitable for clinical and research use (38). According to a study by Jiang et al., the CES-D is a trustworthy and valid three-factor instrument with a Cronbach Alpha value of 0.87 for assessing subthreshold depression in Chinese university students (39). The American validation study was conducted with 1,233 participants who were middle-aged American adults, and a Cronbach's alpha of .90 was obtained. In addition, the 4-factor model had the best model fit (40). Stahl et al. found the CES-D scale to be a reliable instrument in a validation study of 522 multiethnic diabetes patient groups in Singapore (41). It has been found that the Italian translated version of the scale was valid and reliable to be used (24). Also, Cronbach's alpha of the short form of the CES-D scale among Chinese adults was 0.78-0.79, meaning that the scale was valid and reliable (25). A Spanish trial checking the validity and reliability of the CES-D found Cronbach's alpha 0.9 and reported that the scale was valid and reliable (26-30).
Furthermore, another study conducted by Zhang et al. resulted in the Cronbach's Alpha 0.90 for the scale and found that the scale is valid and reliable to use in different ages among the urban population of China (31). In examining studies with various patient populations, the CES-D screening instrument is reliable and valid for assessing depression in stroke patients, HCV patients, and cancer patients (42-44). In a validity study on 102 female and 102 male Canadian military peacekeepers, CES-D was usable for several different measures (45).
Item No. 7 of the scale was omitted from the structure due to its complexity and understandability problem among the population in Afghanistan. It was also omitted in some other studies by Yang et al. to achieve a valid structure and present best-fitted items for the version of the CES-D scale (32).
The CMIN/df for the confirmatory factor analysis was 4.363, which is lower than the result found by Radloff LS and McCauley et al.; however, the Chi-Square/df found in this study is permissible. In addition, the CFI was found to be 0.833 in this study which is also permissible and shows a good fit (8, 33).
This study resulted in the Dari version of the CES-D scale being reliable among Dari speakers in Herat province in Afghanistan. In addition, the Spearman-Brown correlation coefficient was found to be 0.722, which is an acceptable score to show the reliability of a scale.
5. Limitations
This survey was conducted among native Dari speakers living in Herat Province, Afghanistan. To apply the Dari version of the CES-D scale among Dari speakers from all over Afghanistan, more studies covering the country's general population would need to be conducted. The data in this study were collected in Herat province, the second-largest city in Afghanistan. The researchers are recommended to conduct the study in a larger universe by expanding it to different provinces.
Due to the high percentage of illiterate people, we had to read out the questions and record the participants' answers. Many illiterate people make it difficult to claim that residents of Herat province in Afghanistan can fully understand the items on the scale. However, the inherent limitations of using self-report scales should always be considered.
6. Conclusion
This study resulted that the Dari version of the CES-D scale is valid and reliable to use among the general population of Herat province of Afghanistan. The scale can be used to assess depression and its symptoms among the above-mentioned population with confidence.
7. Ethical approval and consent to participate
Ethical approval was obtained from the AMSA Medical Research Center Ethical Committee on 2nd May 2021. During the initial contact with the participants, a description of the study was presented to them. All participants in this study were required to sign a written consent form.
8. Availability of data and materials
On reasonable request, the corresponding author will provide the datasets used in and/or analyzed during the current work.
9. Competing Interest
The authors declare that they have no competing interests.
10. Funding
The research received no external funding.
11. Author contribution
All the authors contributed to designing the conception of the study. AN contributed to data collection and data entry as well as data analysis and data interpretation. AN, NT and FH contributed to drafting the article. All the authors gave the final approval of the version to be published and agreed to be accountable for all aspects of the work.
12. Acknowledgment
We would like to express our sincere gratitude to all the participants who enrolled in this study as well as the Global Health Focus team for their help and guidance.
13. References
- Depression [Internet]. Who.int. [cited 31 December 2021]. Available from: https://www.who.int/news-room/fact-sheets/detail/depression
- Depression and Other Common Mental Disorders [Internet]. Apps.who.int. [cited 31 December 2021]. Available from: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf
- Robins LN, Price RK. Adult disorders predicted by childhood conduct problems: results from the NIMH Epidemiologic Catchment Area project. Psychiatry. 1991 May 1;54(2):116-32.
- Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Archives of general psychiatry. 1994 Jan 1;51(1):8-19.
- Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, Rush AJ, Walters EE, Wang PS. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). Jama. 2003 Jun 18;289(23):3095-105.
- Cuijpers P, Smit F. Subthreshold depression as a risk indicator for major depressive disorder: a systematic review of prospective studies. Acta psychiatrica scandinavica. 2004 May;109(5):325-31.
- Ferrari AJ, Charlson FJ, Norman RE, Patten SB, Freedman G, Murray CJ, Vos T, Whiteford HA. Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS medicine. 2013 Nov 5;10(11):e1001547.
- Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Applied psychological measurement. 1977 Jun;1(3):385-401.
- Lim GY, Tam WW, Lu Y, Ho CS, Zhang MW, Ho RC. Prevalence of depression in the community from 30 countries between 1994 and 2014. Scientific reports. 2018 Feb 12;8(1):1-0.
- Bromet E, Andrade LH, Hwang I, Sampson NA, Alonso J, De Girolamo G, De Graaf R, Demyttenaere K, Hu C, Iwata N, Karam AN. Cross-national epidemiology of DSM-IV major depressive episode. BMC medicine. 2011 Dec;9(1):1-6.
- Davis AK, Barrett FS, May DG, Cosimano MP, Sepeda ND, Johnson MW, Finan PH, Griffiths RR. Effects of psilocybin-assisted therapy on major depressive disorder: a randomized clinical trial. JAMA psychiatry. 2021 May 1;78(5):481-9.
- Chow W, Doane M, Sheehan J, Alphs L, Le H. Le H. Economic burden among patients with major depressive disorder: an analysis of healthcare resource use, work productivity, and direct and indirect costs by depression severity. Am J Manag Care. 2019;16:e188-96.
- Wang PS, Simon G, Kessler RC. The economic burden of depression and the cost‐effectiveness of treatment. International journal of methods in psychiatric research. 2003 Feb;12(1):22-33.
- Shafer AB. Meta‐analysis of the factor structures of four depression questionnaires: Beck, CES‐D, Hamilton, and Zung. Journal of clinical psychology. 2006 Jan;62(1):123-46.
- Jiang L, Wang Y, Zhang Y, Li R, Wu H, Li C, Wu Y, Tao Q. The reliability and validity of the center for epidemiologic studies depression scale (CES-D) for Chinese university students. Frontiers in psychiatry. 2019 May 21;10:315.
- Callahan CM, Wolinsky FD. The effect of gender and race on the measurement properties of the CES-D in older adults. Medical care. 1994 Apr.
- Schroevers MJ, Sanderman R, Van Sonderen E, Ranchor AV. The evaluation of the Center for Epidemiologic Studies Depression (CES-D) scale: depressed and positive affect in cancer patients and healthy reference subjects. Quality of life Research. 2000 Nov;9(9):1015-29.
- Alemi Q, Stempel C, Koga PM, Montgomery S, Smith V, Sandhu G, Villegas B, Requejo J. Risk and protective factors associated with the mental health of young adults in Kabul, Afghanistan. BMC psychiatry. 2018 Dec;18(1):1-0.
- Tomlinson M, Chaudhery D, Ahmadzai H, Rodríguez Gómez S, Bizouerne C, van Heyningen T, Chopra M. Identifying and treating maternal mental health difficulties in Afghanistan: A feasibility study. International journal of mental health systems. 2020 Dec;14(1):1-8.
- Shayan NA, Azizi AT, Razaqi N, Afzali H, Neyazi A, Waez H, Noormohmmadi M, Bhattacharya S. Phase wise assessment of COVID-19 related depression, anxiety, and stress level among patients in Herat city, Afghanistan-A descriptive study. Razi International Medical Journal. 2021 May 24;1(1).
- Lopez VC, de Esteban Chamorro T. Validity of Zung's Self-Rating Depression Scale. Archivos de neurobiologia. 1975 May 1;38(3):225-46.
- Xu MY. Using the SDS (self-rating depression scale) for observations on depression. Zhonghua hu li za zhi= Chinese journal of nursing. 1987 Apr;22(4):156-9.
- Chen XS. Masked depression among patients diagnosed as neurosis in general hospitals. Zhonghua yi xue za zhi. 1986 Jan;66(1):32-3.
- Fava GA. Assessing depressive symptoms across cultures: Italian validation of the CES‐D self‐rating scale. Journal of Clinical Psychology. 1983 Mar;39(2):249-51.
- Boey KW. Cross‐validation of a short form of the CES‐D in Chinese elderly. International journal of geriatric psychiatry. 1999 Aug;14(8):608-17.
- Roberts RE. Reliability of the CES-D scale in different ethnic contexts. Psychiatry research. 1980 May 1;2(2):125-34.
- Garcia M, Marks G. Depressive symptomatology among Mexican-American adults: an examination with the CES-D Scale. Psychiatry research. 1989 Feb 1;27(2):137-48.
- Golding JM, Aneshensel CS, Hough RL. Responses to depression scale items among Mexican‐Americans and non‐Hispanic Whites. Journal of Clinical Psychology. 1991 Jan;47(1):61-75.
- Guarnaccia PJ, Angel R, Worobey JL. The factor structure of the CES-D in the Hispanic Health and Nutrition Examination Survey: the influences of ethnicity, gender and language. Social science & medicine. 1989 Jan 1;29(1):85-94.
- Liang J, Tran TV, Krause N, Markides KS. Generational differences in the structure of the CES-D scale in Mexican Americans. Journal of Gerontology. 1989 May 1;44(3):S110-20.
- Zhang J, Wu ZY, Fang G, Li J, Han BX, Chen ZY. Development of the Chinese age norms of CES-D in urban area. Chinese Mental Health Journal. 2010 Feb.
- Yang L, Jia CX, Qin P. Reliability and validity of the Center for Epidemiologic Studies Depression Scale (CES-D) among suicide attempters and comparison residents in rural China. BMC psychiatry. 2015 Dec;15(1):1-8.
- McCauley SR, Pedroza C, Brown SA, Boake C, Levin HS, Goodman HS, Merritt SG. Confirmatory factor structure of the Center for Epidemiologic Studies-Depression scale (CES-D) in mild-to-moderate traumatic brain injury. Brain Injury. 2006 Jan 1;20(5):519-27.
- Mogos MF, Beckstead JW, Kip KE, Evans ME, Boothroyd RA, Aiyer AN, Reis SE. Assessing longitudinal invariance of the Center for Epidemiologic Studies-Depression Scale among middle-aged and older adults. Journal of Nursing Measurement. 2015 Jan 1;23(2):302-14.
- Center for Epidemiological Studies Depression Scale (CES-D and CES-D-10) - Spinal Cord Injury Research Evidence [Internet]. Spinal Cord Injury Research Evidence. [cited 26 April 2022]. Available from: https://scireproject.com/outcome-measures/list-sci/mental-health/center-for-epidemiological-studies-depression-scale-ces-d-and-ces-d-10
- Schumacker RE, Lomax RG. A beginner's guide to structural equation modeling. psychology press; 2004 Jun 24.
- Shafer AB. Meta‐analysis of the factor structures of four depression questionnaires: Beck, CES‐D, Hamilton, and Zung. Journal of clinical psychology. 2006 Jan;62(1):123-46.
- Fountoulakis K, Iacovides A, Kleanthous S, Samolis S, Kaprinis SG, Sitzoglou K, St Kaprinis G, Bech P. Reliability, validity and psychometric properties of the Greek translation of the Center for Epidemiological Studies-Depression (CES-D) Scale. BMC psychiatry. 2001 Dec;1(1):1-0.
- Jiang L, Wang Y, Zhang Y, Li R, Wu H, Li C, Wu Y, Tao Q. The reliability and validity of the center for epidemiologic studies depression scale (CES-D) for Chinese university students. Frontiers in psychiatry. 2019 May 21;10:315.
- Cosco TD, Prina M, Stubbs B, Wu YT. Reliability and validity of the Center for Epidemiologic Studies Depression Scale in a population-based cohort of middle-aged US adults. Journal of nursing measurement. 2017 Jan 1;25(3):476-85.
- Stahl D, Sum CF, Lum SS, Liow PH, Chan YH, Verma S, Chua HC, Chong SA. Screening for depressive symptoms: validation of the center for epidemiologic studies depression scale (CES-D) in a multiethnic group of patients with diabetes in Singapore. Diabetes Care. 2008 Jun 1;31(6):1118-9.
- Shinar D, Gross CR, Price TR, Banko M, Bolduc PL, Robinson RG. Screening for depression in stroke patients: the reliability and validity of the Center for Epidemiologic Studies Depression Scale. Stroke. 1986 Mar;17(2):241-5.
- Clark CH, Mahoney JS, Clark DJ, Eriksen LR. Screening for depression in a hepatitis C population: the reliability and validity of the Center for Epidemiologic Studies Depression Scale (CES‐D). Journal of Advanced Nursing. 2002 Nov;40(3):361-9.
- Hann D, Winter K, Jacobsen P. Measurement of depressive symptoms in cancer patients: evaluation of the Center for Epidemiological Studies Depression Scale (CES-D). Journal of psychosomatic research. 1999 May 1;46(5):437-43.
- Boisvert JA, McCreary DR, Wright KD, Asmundson GJ. Factorial validity of the center for epidemiologic studies‐depression (CES‐D) scale in military peacekeepers. Depression and Anxiety. 2003;17(1):19-25.