- Available
- XML
- Download citation
- Statistics
- Share




Knowledge, Attitude, And Practices (KAP) Of Malaria Prevention Amongst Medical Students of Obafemi Awolowo University, Ile-Ife, Osun State, Nigeria
show more
| Received 01 May 2022 |
Accepted 09 Nov 2022 |
Published 30 Nov 2022 |
Abstract
Background: Malaria remains one of the foremost causes of morbidity in the world. Practices of preventive measures have been linked to factors including educational status. Students of health-related sciences are expected to possess a high-level knowledge of the disease and translate this into the better practice of preventive measures. Hence, this study was conducted to assess the knowledge attitude and practice of malaria prevention among medical students of Obafemi Awolowo University, Ile-Ife, Osun State, Nigeria.
Methods: Data for this cross-sectional study was collected from 253 consenting medical students using an online group-designed Google Form questionnaire and analyzed using Microsoft excel.
Results: Although 47.83% of respondents think malaria is a deadly disease and 98.81% affirmed it is preventable, almost all (≥98.42%) reported female anopheles’ mosquito and plasmodium as vector and causative agent, respectively. Moreover, 65.22% were very willing to use one or a combination of malaria preventive methods. Insecticides usage were most common among the respondents, with 84.58% having used them in the last year. In contrast, only 12.25% and 35.97% had used Indoor Residual Spray (IRS) and insecticide-treated mosquito net (ITN), respectively.
Conclusion: This study revealed good knowledge and attitude amongst the medical students. However, this did not translate to practice, especially with the most advanced vector control practices such as ITN usage and IRS. Hence, a review of the public/community health curricula and related course modules to provide more information about IRS is recommended. Also, and there is a need for the government to make ITNs more readily available and affordable.
Keywords: Knowledge, Attitude, Practices, Malaria prevention, Medical students, University undergraduates, Osun State, Nigeria.
1. Introduction
Malaria remains one of the foremost causes of morbidity in the world. The World Health Organization reports an estimated 241 million malaria cases and 627,000 deaths worldwide in 2020 (1) . With an estimated 1.38 billion people at risk of infection today, malaria remains one of the significant tropical health challenges in the world (2). It is a vector-borne infectious disease transmitted by female Anopheles mosquitoes, which carry the infective sporozoite stage of the Plasmodium parasite in their salivary glands (3). Both environmental factors and the socio-demographic environment play a role in breeding the female Anopheles mosquitoes and the prevalence of the disease (4,5).
Previous studies have reported that although it is better and cheaper to prevent malaria than manage it, malaria prevention is usually low and difficult to implement when the risk is perceived as low (6,7). Besides, malaria prevention is connected to people's religious preferences and educational background (3,8). However, various methods have recently been used to prevent malaria, with more recent emphasis on vector control. Also, the use of ITNs and IRS has increased over the years in Sub-Saharan Africa, reducing the proportion of the population at risk of the disease (9).
A study on knowledge and practice of malaria prevention and management among non-medical students of the University of Nigeria, Nsukka, revealed a strong relationship between the faculty of the students and their knowledge of malaria. The highest level of knowledge was seen amongst students in the faculty of agriculture, which could be due to their science background (9). Another study on knowledge and practice of malaria prevention methods among nursing and midwifery students in Plateau State, North Central Nigeria, revealed that 85.0% of respondents used ITNs, 58.8% of them used Insecticide Spray, and 54.9% of them used window nets as a means of malaria prevention. Moreover, 73.2% of respondents had high knowledge of malaria prevention due to their field of study in health care (10).
During their training, medical students receive much information concerning malaria and attend to patients affected by the disease. Thus, it is often expected that the intensive training they undergo will contribute to their KAP of malaria prevention. But unlike their non-medical colleagues, the information on the KAP of malaria prevention amongst medical students in Nigeria is inadequate. For as much as we know, this study is the first in Nigeria to assess the KAP of malaria prevention amongst medical students in Nigeria. Hence, this study seeks to assess medical students of Obafemi Awolowo University on their knowledge of the causes, symptoms, and transmission of malaria, habits of mosquito vectors, attitude towards prevention, and prevention practices.
2. Materials and Methods
This study was a quantitative cross-sectional study and formative plan to describe the KAP of malaria prevention amongst medical students. The research was a purposive sampling school-based study carried out among medical students ranging from 100 Level (first-year students) to 600 Level (sixth-year students) of Obafemi Awolowo University, Ile-Ife, Osun State, Nigeria. Medical students, in this regard, refer to students of the Faculty of Clinical Sciences, College of Health Sciences, Obafemi Awolowo University, Ile-Ife.
From a population size of 698 medical students, qualified students (age 15 and above) were recruited for the study and randomly interviewed using a standard questionnaire via Google Forms. Using a confidence level of 98%, a margin error of 5, and a population proportion of 50%, we arrived at a sample size of 249 students. The group-designed Google Form questionnaire was made of close-ended questions and pre-tested by the authors before administering to respondents.
The questionnaire was divided into six sections to collect data from the study population on their consent, demographics, knowledge about the symptoms and causes of malaria, knowledge regarding malaria transmission and habits of the mosquito vector, knowledge and attitude towards malaria prevention, and practices of prevention of malaria. The collated data was cross-tabulated and analyzed as frequencies and percentages using Microsoft excel (2010 version).
The prerequisite for conducting studies that involve human participation was followed. Confidentiality and ambiguity were ensured, and the right to withdraw from the studies was reprised.
3. Results
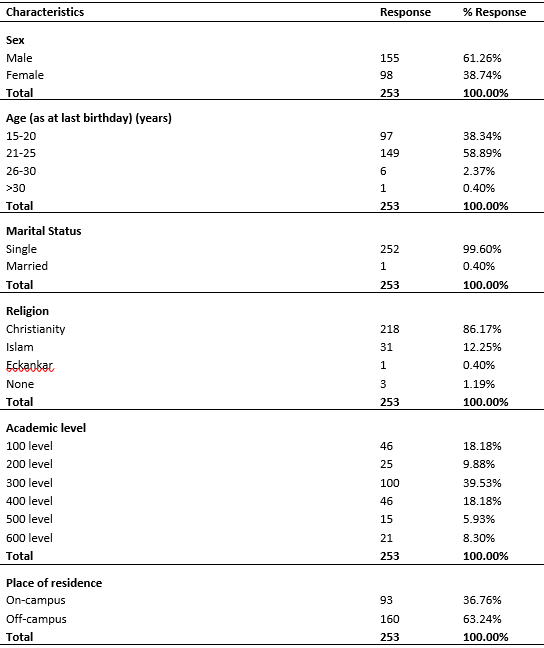
The study had a total of 253 participants who are medical students of Obafemi Awolowo University, Ile-Ife, Osun State, Nigeria. Of this total number of participants, 155 (61.26%) were males, while 98 (38.74%) were females. The participants ranged from 15 years and above, with the highest number of participants being between the age of 21 to 25 years. Based on the marital status of respondents, almost all respondents (99.60%) were unmarried. Also, a greater percentage of respondents (86.17%) are Christians by religion. On the academic level of participants, 39.53% are at 300 Level, and 5.93% are at 500 Level. In contrast, the rest of the participants are relatively distributed in other levels, as indicated in Table 1 below. 63.24% (n=160) lived outside the campus compared to 36.76% (n=93) who stayed within the campus.
On the knowledge of the causes and symptoms of malaria outlined in Table 2 below, 3.56% (n=9) had never been sick with malaria. In comparison, 28.06% had been diagnosed with malaria once in the past year. While 47.83% (n=121) of the respondents perceived malaria as a deadly disease, 39.13% perceived it as an ordinary disease. The most familiar signs and symptoms of malaria experienced by respondents include headache, fever, chills and shivering, joint and body pains, nausea and vomiting, and dizziness. A smaller number of participants, however, experienced other symptoms such as blister of the mouth and a bitter taste. 98.42% of the participants identified the cause of malaria as the bite of infected female anopheles’ mosquitoes.

On the knowledge of the transmission of malaria and the habits of the mosquito vector (Table 3), Almost all (99.6%) participants identified that the mode of transmission of malaria is the bite of infected mosquitoes. All participants (100%) identified the female anopheles' mosquito as the malaria vector. Nearly all (98.42%) participants identified that the plasmodium parasite is the causative agent of malaria, and more than half (55.73%) believed that they usually bite at night. Almost all of the participants (99.21%) identified that stagnant water is the common breeding site for the malaria vector and dirty places were the most common (41.11%) resting site for the malaria vector.

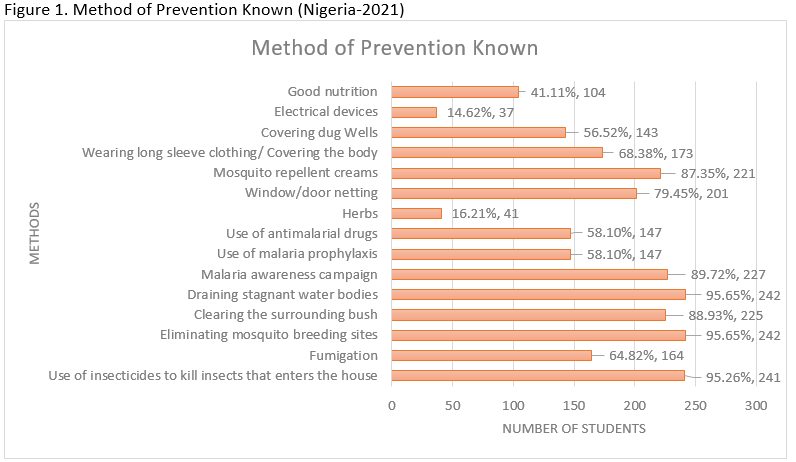
In table 4 below, almost all (98.81%) participants affirmed that malaria is preventable. These respondents identified the use of insecticides, elimination of breeding sites of mosquitoes, draining of stagnant water bodies, clearing of surrounding bushes, malaria awareness campaigns, use of mosquito repellent creams, and fumigation strategy as ways of preventing malaria (Figure 1). One hundred seventy-six respondents had not heard of IRS. In contrast, out of the 77 participants that have heard about it, only 61.04% (n=47) have used the IRS before.

Looking at the efforts to prevent malaria (Table 5), 165 (65.22%) participants were very willing, and 31.62% were willing to use one or a combination of the preventive methods for malaria. This willingness is seen in 84.58% of 253 students who have used insecticides, 35.97% of participants who slept under ITNs and 12.25% who had used IRS (Figure 2). However, 67.59% of the participants combined the use of insecticides with the ITNs. About 34.78% of the students have never slept under an ITN, and frequent usage of ITNs was discovered to be approximately 2%. About 43% of participants used insecticides at least once a month compared to 1.58% that utilized insecticides daily. Most of the respondents (77.08%) made use of repellent creams; among those individuals, the regular use interval was once a week in some respondents (n=16). It was impressive to see that 85.77% of these students take care of their surroundings in the light of overgrown bushes and 75.10% engaged in removing stagnant water, 56.92% conducted this bush-clearing exercise monthly, 25.30% and 28.06% attended to stagnant water daily and weekly respectively. Malaria prophylaxis medications were consumed by 67.19%, and wearing clothes with more cover was not appreciated by 20.16%. However, about 60% used Mosquito door nets. Burning of waste was the most preferred choice of discarding household waste by about half of the students (52.57%) as compared to the use of an outdoor disposal method (18.58%) and drainage channel (28.85%).

4. Discussion
Menstruation is a normal physiological process in females that is part of pubertal development. Adequate knowledge and good menstrual practice are required to prevent adverse reproductive health outcomes and poor academic performance in adolescent school girls (15, 17). In this cross-sectional study among secondary school girls in Herat city, only 39.2% of the participants heard about menstruation before menarche. In the general population, no one mentions the name of genital parts, although a part of the human body, it would be considered impoliteness. This practice reflects the socio-cultural beliefs and norms attributed to menstruation and the female reproductive organs. Dissimilarly, a study of secondary school girls in Nigeria showed that 96.4% of girls heard about menstruation before experiencing menarche (15). This difference might be due to the high educational level of the mothers and a close relationship between mother and children attributed to culture. In another related study in Western Ethiopia and Northeast Ethiopia, 79.3% and 86.7% of girls heard about menstruation before menarche, respectively (18-19). In comparison, most of the girls in this study have poor knowledge on menstruation when they experience menarche, thus making menarche a bad and fearful experience for them.
Regarding the severity of the disease, about one-third (39.13%) of our study population believe malaria is an ordinary disease. In comparison, a significant number (7.51%) are unsure whether it is deadly or ordinary. This finding disagrees with a similar study amongst non-medical students in Kwara State, where 54.05% agreed malaria is an ordinary disease and 3.86% were not clear (17). But this variation can be linked to medical students' good knowledge of malaria due to their training relative to their non-medical counterparts.
We also found that almost all (≥88.93%) of our study population believe the female Anopheles mosquito is the vector for malaria, the bite of an infected mosquito is the commonest mode of transmission; plasmodium as the causative agent; stagnant water is the commonest breeding site for the vector; and headache, chills and shivering, and fever are signs and symptoms of malaria. This finding agrees with other studies in malaria-endemic regions in Nigeria, Kenya, Ethiopia, and Guatemala, which is unsurprising since they have ruled that knowledge about malaria is widespread in endemic regions (6,10,18–22). But it disagrees with other studies, especially on the bite of infected female Anopheles mosquito as the cause of malaria (11,16,23).
Moreover, we found that a sizeable portion (96.44%) of our study population often get diagnosed with malaria at least once a year. This finding is not surprising since the study area is a malaria-endemic region (6). Therefore, the excellent knowledge of signs and symptoms of malaria seen in our study population could be said to be from personal experiences during their previous malaria infections, which is in keeping with previous studies. Interestingly, this might be a source of concern in that cases of self-diagnosis and self-treatment have been reported as prevalent amongst malaria-endemic populations and populations with good knowledge of malaria signs and symptoms (24,25). Unfortunately, while our study reported high (67.19%) use of antimalarial drugs, we did not probe further into cases of self-diagnosis and self-treatment. We, therefore, recommend a future study to look into this.
Our study population demonstrated good knowledge, and attitude towards malaria prevention as almost all (98.81%) agree that malaria is preventable, which is in keeping with findings in previous studies (9,11,14,26). This finding may not be unconnected to the general public awareness of the preventability of malaria and the literacy of our study population, which provides evidence to corroborate previous studies that have established that people's education level strongly influences their knowledge and attitude towards malaria (3,8,14).
In addition, more than two-thirds (≥95.26) of our study population selected the use of insecticides, draining stagnant water bodies, and eliminating mosquito breeding sites as a method of prevention. This finding amplifies findings in previous studies (6,10,14,27). It provides evidence that partly supports the possible effectiveness of these methods, as suggested in a previous study which gives a historical analysis of the evidence and strategies for malaria prevention and control (27). This wide synergy is not surprising since the study areas are malaria-endemic, and malaria awareness messages are spread readily. Moreover, very few (14.62%) of our study population indicated electrical devices as a prevention method. Generally, electronic devices are ineffective preventive methods (28). Hence, this could be the reason for having the lowest selection on the list.
Despite the population's good knowledge and attitude, an unexpected higher infection rate is seen as more than two-thirds (68.38%) of them have had malaria at least once in the last six months. Ordinarily, this should not be a source of concern as previous studies have established that malaria is prevalent in the study area (6,24). A similar high infection rate has been reported in other studies (9,29). But for our population that has demonstrated good knowledge and attitude towards malaria prevention, it is worrisome.
Interestingly, this unfortunate reality could be due to several reasons, one of which could be that our study population, who are medical students, do not practice malaria preventive measures as religiously as their non-medical counterparts, especially since they are very knowledgeable and can easily self-diagnose when they get infected. This postulation might not be a hard-found fact, as a previous study in our study area has ruled that many undergraduates diagnose themselves with malaria from their response to specific symptoms such as fever, weakness, headache etc (24). As a sequel to this self-diagnosis, it could be that our study population got used to malaria and thus perceived it as a trivial issue (6). So, they now regularly treat themselves with the use of antimalarials, and this is in keeping with earlier studies that have reported self-treatment with antimalarial drugs as a common phenomenon amongst endemic populations (30–33.) Then, their body systems start to resist these antimalarial drugs over time, which fuels a self-sustaining cycle of continued usage. Although this is problematic as well, it is not surprising as malaria-endemic populations are generally known to have a low compliance rate to completing the dosage of their antimalarial drugs, which is corroborated by a similar study in Turkey, where about half of the study population was reported not to finish their dosage even when the government made antimalarial drugs available to them for free (34).
We also found that of the less than one-third (30.43%) of the study population that has heard of IRS before, only about two-thirds (61.03%) of them have used it. IRS is a practice of spraying insecticides on the inner walls of the house and remains an acceptable preventive method for malaria (26). Hence, it is surprising that most of our study population, who should be more knowledgeable about the most advanced malaria prevention practices, have not heard about it before. Interestingly, previous studies amongst non-medical students’ report that about half (≥47.7%) of them had heard of IRS (9,11,26). They have regarded this knowledge level as poor and suggested that the reason for this could be the nature of the educational curricula of the non-medical students (11).
Generally, the low level of knowledge of IRS might be due to the technicalities and relatively high cost involved in the deployment of IRS, as noted in an adjusted twenty-year retrospective analysis of Sub-Saharan Africa (35). However, although both are poor, the higher level of awareness amongst non-medical students than medical students present a paradoxical reality suggesting that the earlier identified deficient educational curricula might not sufficiently explain or justify. We, therefore, recommend it to other researchers for a future study as it does not conveniently fit into the scope of this study.
Our study revealed that almost all (96.84%) of our study population were (very) willing to use listed malaria preventive methods. Correspondingly, our study population had very high insecticide use as almost all (84.58%) had used it in the last year, and only a few (15.81%) had never used it. However, in sharp contrast to the more than two-thirds of our study population that use antimalarial drugs/malaria prophylactics (67.19%) or repellent creams (77.08%), our study revealed poor usage of ITNs. Only about a third (35.97%) of our study population had used ITNs over the last year, while about an equal number (34.78%) had never used ITNs.
This finding of poor usage of ITNs agrees with similar studies in Ondo, Osun, and Cross-River States, where ITN usage was significantly lower (6,11,26,36). But it disagrees with other studies in Enugu and Plateau States, where ITN usage was much higher, and use of insecticides was lower (9,10). The Enugu State study, while comparing their findings with previous studies in Osun and Cross-River States, has suggested that the higher level of usage of ITNs amongst their study population might be due to their higher level of education (9,11,36). However, our findings defy this line of thought in that a lower level of usage is seen amongst our study population, who are expected to have a better knowledge of malaria prevention. Hence, there might be evidence to support that although their suggestion might be valid to an extent, the relationship between the literacy level and low usage of ITNs might not be a direct one.
Unfortunately, this study did not assess the likely reasons for the low usage of ITNs. But the sharp contrast with the very high usage of relatively cheaper insecticides might be enough to suggest the high cost of purchasing ITNs, and previous studies support this (6,9,12). Moreover, our study population consists of students, many of whom are not gainfully employed and may belong to the low-income socioeconomic strata of the society. Hence, as reported in a Malawian study that low-income households spend less on malaria prevention when compared to their high-income household counterparts, we can safely predict that our study population might not have sufficient income to procure these ITNs (37). Also, compared to the high willingness to use these malaria preventive methods, including ITNs, we can conclude that the unavailability of ITNs is another reason for their poor usage, as noted in previous studies (6,9,12). This is, therefore, a clarion call for the government at all levels to urgently consider making ITNs available for the Nigerian populace at a very affordable cost (9).
Similarly, our finding that a sizeable portion (67.19%) of the study population use preventive drugs/antimalarial drugs/malaria prophylactic is consistent with another study in Ekiti State, where 59% of the study population admitted to using prophylactic malaria drugs (14). But it differs from others in Enugu and Oyo States, where awareness level was much lower, although they didn't report usage (9,38). Malaria prophylactics are not recommended for endemic populations like Nigerians (9). Hence, the low awareness level is not unexpected. But the high level of usage amongst our study population, which is commensurate with the high infection rate, suggests that they probably engage in self-diagnosis and self-treatment, owing to their excellent knowledge about malaria. And since malaria prophylactics are cheaply sold over-the-counter, they find it very easy to purchase them. Therefore, this provides evidence to support a call for more emphasis on ITN usage and environmental hygiene and less on using malaria prophylactics as effective preventive measures (9).
Furthermore, compared to previous studies, the increased awareness and willingness to use malaria preventive methods amongst our study population attributable to their training underscores malaria awareness campaigns as an effective way of promoting malaria prevention. This finding is corroborated by a significantly large number (89.72%) of our study population recommending it, as noted in similar studies (6,26).
Our study also found that most of the study population clear bushes in their surrounding/environment and wear long-sleeve clothing as part of malaria preventive efforts. Generally, these may not be perfect malaria preventive measures, especially for future healthcare workers (6). But it is a pointer to practices of personal hygiene and environmental sanitation amongst the population, which is commendable. Also, with more than two-thirds (71.15%) of our study population admitting to disposing of household waste by burning or dumping it in an open space, there is evidence to suggest a hypothesis that practices of medical students contribute to global warming and environmental pollution. Given these impacts on the health of living things, this paradoxical reality might also interest other researchers.
6. Limitations
This study only justifies the KAP of malaria prevention amongst medical students in Obafemi Awolowo University, Ile-Ife, Osun State. Therefore, this study might not be representative of all medical students in Nigeria. However, during the study, we faced barriers that made us unable to verify the validity of the reported malaria diagnosis. Also, this study did not examine other factors which may have contributed to high malaria incidence despite their knowledge of malaria.
7. Conclusion
In conclusion, we found that medical students have a good knowledge and attitude towards malaria prevention, which is expected, given their training. However, this good knowledge and attitude did not translate to practice, especially concerning the most advanced vector control practices such as ITN usage and IRS.
8. Recommendations
We recommend a review of the public/community health or community medicine curricula and related course modules with elements of public health and disease prevention to provide more information about IRS for medical students and their non-medical counterparts. We also call on the government and all stakeholders to step up on malaria awareness campaigns while making ITNs more readily available and affordable.
9. Acknowledgements
We appreciate the students for their participation.
10. Funding
None.
11. Competing Interests
The authors declare no competing interests.
12. Contributions
All authors contributed equally to preparing questionnaires, reviewing the literature, analyzing data, writing the draft, and reviewing the manuscript. However, Matthew Temitayo Femi and Komolafe Olaitan Deborah further contributed to data collection.
13. References
- World Health Organization. Malaria [Internet]. 2022 [cited 2022 Jul 10]. Available from: https://www.who.int/news-room/fact-sheets/detail/malaria
- Carrera LC, Victoria C, Ramirez JL, Jackman C, Calzada JE, Torres R. Study of the epidemiological behavior of malaria in the Darien Region, Panama. 2015-2017. PLoS ONE. 2019 Nov 15;14(11).
- Okwa OO, Soremekun B M, Adeseko O, Raheem A M. Artisans and traders’ knowledge, attitude and practices of malaria in selected areas of Lagos, Nigeria. Global Advanced Research Journal of Medicine and Medical Sciences. 2012;1(3).
- Hay SI, Guerra CA, Gething PW, Patil AP, Tatem AJ, Noor AM, et al. A world malaria map: plasmodium falciparum endemicity in 2007. PLoS Medicine. 2009 Mar;6(3):0286–302.
- Ibor UW, Okoronkwo EM. Demographic and Socioeconomic Factors Influencing Malaria incidence in Calabar, Cross River State, Nigeria. Science World Journal. 2017;12(3):19–24.
- Erhun W, Agbani E, Adesanya SO. Malaria prevention: knowledge, attitude and practice in a Southwestern Nigerian community. African Journal of Biomedical Research. 2005;8(1):25–9.
- Winch PJ, Makemba AM, Kamazima SR, Lwihula GK, Lubega P, Minjas JN, et al. Seasonal Variation in the Perceived Risk of Malaria: Implications for the Promotion of Insecticide-Impregnated Bed Nets. Sot Sci Med. 1994;39(1):63–75.
- Dike N, Onwujekwe O, Ojukwu J, Ikeme A, Uzochukwu B, Shu E. Influence of education and knowledge on perceptions and practices to control malaria in Southeast Nigeria. Social Science and Medicine. 2006 Jul;63(1):103–6.
- Anene-Okeke CG, Isah A, Aluh DO, Ezeme AL. Knowledge and practice of malaria prevention and management among non-medical students of university of Nigeria, Nsukka. International Journal Of Community Medicine And Public Health. 2018 Jan 24;5(2):461.
- Appiah S, Danjuma BA, Tolulope AO, Zuwaira HI, Olatunde YK, Olufemi AE, et al. Knowledge and practice of methods of malaria prevention among nursing and midwifery students in Plateau state, North Central Nigeria. International Journal of Biomedical Research. 2017;8(04):215–9.
- Edet-Utan O, Usman SO, Ipinmoye TO, Adu AS, Fadero T. Knowledge and practice of malaria prevention among nonmedical students of higher institutions in Ondo State, Nigeria. International Journal of Innovations in Medical Education and Research. 2015;1(1):15–9.
- Senbanjo IO, Adeodu OO, Ogunlesi TA, Anyabolu CH, Okusanya AA. The use of antimalaria drugs and insecticide treated nets in Ile-Ife, Nigeria. Nigerian Journal of Medicine. 2006;15(3):277–80.
- Dejazmach Z, Alemu G, Yimer M, Tegegne B, Getaneh A. Prevalence of Malaria and Associated Knowledge, Attitude, and Practice among Suspected Patients in Bahir Dar Zuria District, Northwest Ethiopia. BioMed Research International. 2021;2021(1).
- Adegun J, Adegboyega J. Knowledge and the preventive strategies of Malaria among Migrant Farmers in Ado-Ekiti Local Government Area of Ekiti State, Nigeria. American Journal of Scientific and Industrial Research. 2011 Dec;2(6):883–9.
- Salako L A, Brieger W R, Afolabi B M, Umeh R E, Agomo P U, Asa S, et al. Treatment of Childhood Fevers and Other Illnesses in Three Rural Nigerian Communities. Journal of Tropical Paediatrics. 2001 Aug;47(1):230–8.
- Oladepo O, Tona GO, Oshiname FO, Titiloye MA. Malaria knowledge and agricultural practices that promote mosquito breeding in two rural farming communities in Oyo State, Nigeria. Malaria Journal. 2010;9(91).
- Mufutau A, Joseph O, AbdulGafar N, Olayinka S, Femi E, Author C. Knowledge, Attitude and Practices About Malaria Among Members of a University Community in Kwara State, Nigeria. Animal Research International. 2017;14(3):2793–803.
- Okoli CA, Enna MA. A cross-sectional study on knowledge of, attitudes towards and practice of malaria prevention and control measures in central Nigeria. Southern African Journal of Infectious Diseases. 2015 Jul 15;29(1):37–42.
- Jima D, Tasfaye G, Deressa W, Woyessa A, Kebede D, Alamirew D. Baseline survey for the implementation of insecticide treated mosquito nets in Malaria control in Ethiopia. Ethiopian Journal of Health Development. 2005 Jun 24;19(1):16–23.
- Klein RE, Weller SC, Zeissig R, Richards FO, Ruebush TK. Knowledge, beliefs, and practices in relation to malaria transmission and vector control in Guatemala. The American Journal of Tropical Medicine and Hygiene. 1995;52(5):383–8.
- Deressa W, Ali A, Enquoselassie F. Knowledge, Attitude and Practice About Malaria, the Mosquito and Antimalarial Drugs in a Rural Community. Ethiopian Journal of Health Development. 2004 Mar 25;17(2):99–104.
- Okech BA, Mwobobia IK, Kamau A, Muiruri S, Mutiso N, Nyambura J, et al. Use of Integrated Malaria Management Reduces Malaria in Kenya. PLoS ONE. 2008 Dec;3(12).
- Idowu OA, Mafiana CF, Luwoye IJ, Adehanloye O. Perceptions and home management practices of malaria in some rural communities in Abeokuta, Nigeria. Travel Medicine and Infectious Disease. 2008 Jul;6(4):210–4.
- Babalola OO, Lamikanra A. The response of students to malaria and malaria therapy in a university in Southwest Nigeria. Research in Social and Administrative Pharmacy. 2007 Sep;3(3):351–62.
- Curtis CF, Mnzava AEP. Comparison of house spraying and insecticide-treated nets for malaria control. Bull World Health Organ. 2000;78(12):1389–400.
- Isola I, Edet-Utan O, Ojediran T, Usman S. Osun state non-medical students’ perceptions and practice of malaria prevention. Journal of Behavioral Health. 2015 Jul 9;4(1).
- Gachelin G, Garner P, Ferroni E, Verhave JP, Opinel A. Evidence and strategies for malaria prevention and control: A historical analysis. Malaria Journal. 2018 Feb 27;17(1).
- Enayati AA, Hemingway J, Garner P. Electronic mosquito repellents for preventing mosquito bites and malaria infection. Cochrane Database of Systematic Reviews. 2007;(2).
- Sam-Wobo SO, Akinboroye T, Anosike JC, Adewale B. Knowledge and practices on malaria treatment measures among pregnant women in Abeokuta, Nigeria. Tanzania Journal of Health Research. 2008 Oct;10(4):226–31.
- Nuwaha F. People’s perception of malaria in Mbarara, Uganda. Tropical Medicine and International Health. 2002 May;7(5):462–70.
- Foster SD. Reviews/Analyses Pricing, distribution, and use of antimalarial drugs. Bull World Health Organ. 1991;69(3):349–63.
- Ruebush TK, Godoy HA. Community participation in malaria surveillance and treatment: The Volunteer Collaborator Network of Guatemala. The American Journal of Tropical Medicine and Hygiene. 1992;46(3):248–60.
- Yeneneh H, Gyorkos TW, Joseph L, Pickering J, Tedla4 & S. Antimalarial drug utilization by women in Ethiopia: a knowledge-attitudes-practice study. Bull World Health Organ. 1993;71(6):763–72.
- Simsek Z, Kurcer MA. Malaria: Knowledge and behaviour in an endemic rural area of Turkey. Journal of the Royal Institute of Public Health. 2005 Mar;119(3):202–8.
- Tangena JAA, Hendriks CMJ, Devine M, Tammaro M, Trett AE, Williams I, et al. Indoor residual spraying for malaria control in sub-Saharan Africa 1997 to 2017: An adjusted retrospective analysis. Malaria Journal. 2020 Apr 10;19(1).
- Udonwa NE, Gyuse AN, Etokidem AJ. Malaria: Knowledge and prevention practices among school adolescents in a coastal comm unity in Calabar, Nigeria. African Journal of Primary Health Care and Family Medicine. 2010;2(1).
- Ettling M, McFarland DA, Schultz LJ, Chitsulo L. Economic impact of malaria in Malawian households. Tropical Medicine and Parasitology Journal. 1994 Apr;74–9.
- Ibrahim A, Aminat Oluberu O, Usman SO, Akintayo-Usman O, Nafisat Isola I, Ojediran TE, et al. Oyo State Students and Malaria Management. Turkish Journal of Family Medicine and Primary Care. 2016;10(3):126–30.