- Available
- XML
- Download citation
- Statistics
- Share




Management capacity in the Afghan Ministry of Public Health pre-Taliban: A mixed-methods study of political and socio-cultural issues
show more
| Received 04 Jan 2023 |
Accepted 25 Apr 2023 |
Published 30 May 2023 |
Abstract
Background: The importance of management capacity in the health sector has been increasingly recognized. After decades of conflict one of the main obstacles facing the Afghan health system was the limited ‘management/leadership capacity.’ To effectively build capacity it is important to understand the underlying issues.
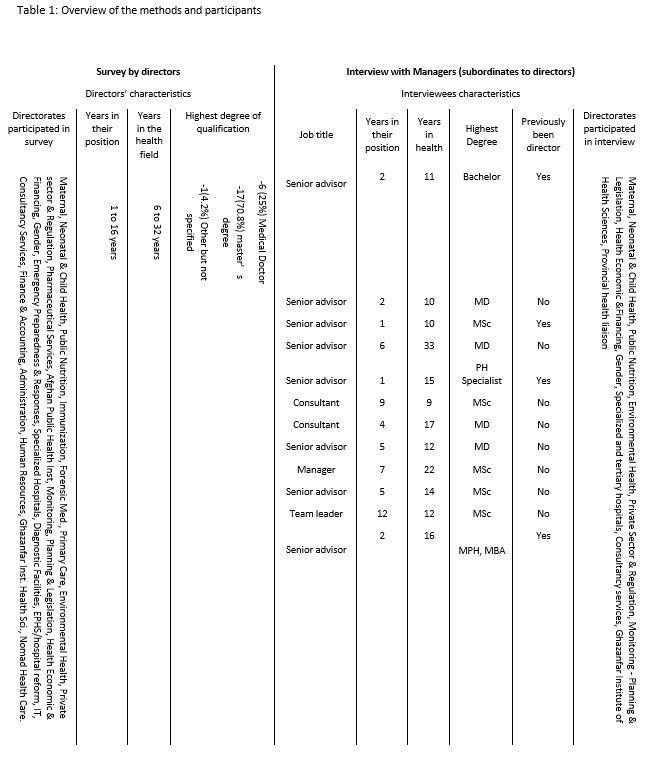
Methods: A mixed-methods study, conducted in 2017/18, before the Taliban takeover, was carried out in all directorates of the Ministry of Public Health (MoPH) to explore the management/leadership capacity. Interviews were conducted with 12 staff; data were analyzed thematically. A quantitative survey was also conducted covering directors of 30 departments, it was analyzed using descriptive statistics.
Results: Our research identified four main factors in the MoPH affecting management and leadership capacity; insufficient support, uncoordinated capacity building, political and socio-cultural issues, and lack of transparency/accountability. This paper focuses on one aspect - the perceptions of the MoPH employees about the impact of political/socio-cultural issues on capacity. Overall, management capacity was weak. Key appointments including directors were subject to political interference and many directors appointed by politicians lacked the required management skills. Consequently, those directors were not able to support employees appropriately or to create a healthy work environment. Overall, there were strong socio-cultural influences such as nepotism and favoritism. Due to these problems employees believed they were not treated consistently or fairly. This was compounded by overly complex administrative systems.
Conclusion: Being able to strengthen management and leadership capacity in the Afghan health system depends largely on the implementation of (existing) anti-corruption strategies.
Keywords: Afghanistan, Management capacity, Health Ministry, Political influence, Socio-Cultural practices.
1. Introduction
The health system in Afghanistan was re-built after the fall of the first Taliban regime in 2002. To deliver a well-coordinated health service, the Ministry of Public Health (MoPH) received financial and technical support from the international community (1). The MoPH had a stewardship role and was responsible for reviewing contract bids, monitoring and evaluation of the implementers’ performance and establishing policies, strategies, and standards (2).
A Basic Package of Health Services (BPHS) and Essential Package of Health Services (EPHS) provided through non-governmental organizations (NGOs) was designed to tackle priority health problems and rapidly expand services throughout the country (3). This resulted in increased access to healthcare for men and for women, increased utilization of services and significant health improvements (4,5). The establishment of midwifery schools in 34 Afghanistan provinces between 2002 and 2013 and the subsequent reduction in maternal mortality was another key achievement of the MoPH (6).
Despite progress, the World Health Organization (WHO) claimed that Afghan health indicators remained worryingly high when regional and global comparisons were made (7). There might be many reasons for this. In Afghanistan, decades of war and the resulting poverty and unemployment can be a root cause of such issues (8). Insecurity, shortage of funds and resources, inadequate numbers of trained staff, especially female healthcare providers, and a dispersed population are other challenges. Another obstacle to national health improvement might be limited capacity at the managerial level (7). Low capacity was recognized as a challenge in 2002 by the MoPH, (9) since then US $ 1.6 billion was spent on capacity building (10), but neither the MoPH nor the partners were satisfied with the management capacity. However, no research has been carried out to explore what factors affected the management and leadership capacity.
The long conflict has weakened government institutions and resulted in severe social and ethnic rifts (8). In addition, some political groups developed economic interests that overrode their original political aims (11). Needs and obligations can cause people to do unwanted things for the survival of their family. This might cause or promote nepotism and compliance with other socio-cultural obligations and slowly it can change behavior (12).
A study was, therefore, carried out to identify what effects the management and leadership capacity and the performance of the organization. As leadership is at the center of the management capacity this study also aimed to understand what role they play in the work environment. The study question was 'What are the factors that affect the management capacity, leadership, and employee performance in the MoPH, Afghanistan?’ The focus of this paper is on the political and socio-cultural issues and the perception of leaders and senior employees on how this affects the management/leadership capacity.
It should be noted that this research was conducted in 2017/18. The health system has changed since then following the takeover by the Taliban in August 2021. It is likely that there are currently limited options for reforms within the MoPH. However, our findings will be beneficial for those working in health systems and public ministries of similar settings.
2. Materials and Methods
A mixed-methods study was appropriate for this in-depth exploration of a complex situation in the MoPH headquarters (13). The directorates were chosen because they direct and monitor the entire health system. Data were collected and analyzed by the first author, who is an Afghan medical doctor. The study was awarded ethical approval by Bournemouth University, UK and the Institutional Review Board, MoPH, Afghanistan (Reference # 43863). Information was provided to participants in Farsi and English explaining their rights to decide whether to participate in the research or not (14). Our study did not measure the MoPH’s performance but rather explored staff views about the MoPH leaders’ capacity and leadership.
Survey
The survey investigated the directors' perception of the management capacity and leadership in the MoPH. Directors were provided both English and Farsi versions of questionnaires (15), (copies available from first author) containing 44 questions about management support, directorate performance, the effects of political and socio-cultural factors and leadership capacity. It was tested by five professionals and minor adjustments were subsequently made (16). Total population sampling was applied including all 30 directorates, and 24 directors completed the questionnaire. Three directors chose not to participate. Two directors had only been in their post for a few months, and one director position was vacant. Due to the low numbers only descriptive statistics are provided.
Interview
Semi-structured interviews, (17) were conducted to explore the perception of other senior staff (subordinates to director) in each directorate about management capacity/leadership and how this affects employee performance. (Copies of questions are available from the first author). The directorate staff were asked to identify the most senior colleagues and those who replied to our email were selected for interview. Three pilot interviews (18) were conducted and the interview schedule was then adapted to address the issues that had identified. Interviews were held in Farsi, digitally recorded, and took between 42-71 minutes. Participants were asked about political and socio-cultural issues and how they affect the employees’ performance. Data saturation was reached at 12 interviews (19). The data analysis was informed by the Braun and Clarke thematic analysis process (20) using NVivo. The result section below amalgamates the survey findings with the themes generated through interview.
3. Results
Our analysis resulted in four factors that affected the management/leadership capacity and the employees’ performance; 1. Insufficient support 2. Uncoordinated capacity building 3. The negative influence of political and socio-cultural issues 4. Lack of transparency and accountability. All factors are interlinked. The focus of this paper is on the political and socio-cultural issues and how they influenced management capacity and organization performance. Political parties are predominantly divided along ethnic lines with linguistic or regional links. The findings revealed that political allegiances are also very influential in the MoPH directorates. It is difficult to separate the political issues from the socio-cultural issues as these two aspects are interconnected in Afghanistan.
Survey analysis
Political interference was identified as the second highest obstacle (81% of respondents;19/24 directors) in achieving the MoPH goals after a shortage of resources (85.7%; 21/24 directors). The government was blamed for allocating key positions along parties/tribal lines. This put people in senior positions without considering whether they had the necessary qualifications and skills as the following quote illustrates:
“Our current state of affairs lies on the political and other discriminations; employment of people is on the basis of political pressures which is an obstacle in reaching our goals” (Participant 6).
Directors reported that socio-cultural issues were another obstacle that negatively affected leadership such as nepotism (the act of using your power or influence to get good jobs or unfair advantages for members of your own family),[21] favoritism (unfair support shown to one person or group, especially by someone in authority)[21] and cronyism (when someone important gives jobs to friends rather than to independent people who have the necessary skills and experience) [21] were major obstacles rated by directors at 80%, 70% and 50% respectively. A few directors who answered that there were no problems affecting their leadership, nevertheless reported nepotism, favoritism and cronyism as obstacles to achieving their goals as directors. Participants were asked to provide their ideas about the solutions for the top obstacles that they faced in reaching their organizational goals. Although participants were directors and could have been introduced by political allies themselves, most suggested that the best solution was to strive against the interference of political pressures, powerful people and other socio-cultural influences.
“Employment of individuals should be on the basis of merit, regardless of ethnic, linguistic, religious or other issues” (Participant 6).
Participants claimed that many of the problems in the MoPH were caused by political and socio-cultural issues; hence they wanted the government to fight against this and not allow political pressure and interference in the health system.
“The government can stop the interference of politics in the MoPH if it develops and implements the law” (Participant 4).
Interview analysis
Almost all interviewees were frustrated by political interference in the MoPH and by favouritism, nepotism, and other socio-cultural influences. The MoPH was under pressure from politicians to hire certain people who were regarded as incompetent. Parliamentarians were even said to interfere in the hiring and firing of people in lower positions. Interviewees claimed that this negatively affected the MoPH performance as the priority was deemed to be political rather than for public benefit as explained below.
“Political interference has taken root in the MoPH. Politicians are destroying the health system of Afghanistan because it runs for the benefit of politicians rather than for the benefit of the public” (Interviewee 2).
Officially, contracts to implement the BPHS and EPHS in the country are awarded to NGOs according to a strict bidding process. However, the quote below indicates that these contracts are awarded to powerful people who were perhaps not motivated to improve the quality of services.
“There are too many problems in public health. People who are powerful won the contracts; people who are powerful are the implementers, people who are powerful are the decision makers, so when weaknesses and gaps are reported, they are considered superficially” (Interviewee 3).
Interviewees explained that political interference was not a new problem, but that it has worsened under the current government. Interestingly, some interviewees thought that there was less political and socio-cultural influence in the MoPH than in other ministries. Some employees were described as caring more about their political allegiances than working for the benefit of the MoPH and the Afghan people.
“…people who come from political parties, for them political aims and benefits are more important than the aims and benefits of the whole of Afghanistan” (Interviewee 11).
Interviewees also said that the MoPH was struggling with the impact of socio-cultural practices. Without relationships and connections (unfair support from people who are in the higher positions), getting support was seen as impossible. The interviewee below claims that this is ubiquitous in the MoPH.
“We are drowning in corruption, it is nothing but these matters; favouritism, nepotism, kinship, personal interests, friendship, political partnerships, family members….” (Interviewee 10).
People needed connections to be hired, appraised well, receive training and to be promoted. From the quote below, it seems that directors had an important role in allowing, perpetuating, or creating this practice in the MoPH.
“During your research, pop up to all the departments and find out when the head of the department was assigned as director and after that, how many of his political party members, tribe and family members were hired in that department. Without much effort, you will find out the reality straightaway” (Interviewee 11).
Interviewees claimed that political pressures and socio-cultural practices had a significant impact on employee performance because this situation created a lack of transparency and accountability. Employees, they said, were treated inconsistently in the provision of all kinds of opportunities including staff development. Interviewees reported a huge difference in the capacity and commitment of employees due to the lack of transparency in the hiring processes which resulted in the appointment of many employees not based on merit. Employees from tribes who were not affiliated to a political party struggled to progress in their careers even if they were competent and knowledgeable. Neither there was a good system of employee performance appraisal as the directors had to give good scores to employees because of social relationships, friendship or to help the employees financially through salary increments rather than award scores based on their performance. In this case good performers were not recognized or rewarded.
The MoPH directors and employees concurred that socio-cultural issues and political interference were one of the significant obstacles to achieving their goals. This resulted in discrimination, inconsistency, unfairness, and lack of transparency as well as the appointment of managers based on political and socio-cultural connections rather than on merit.
4. Discussion
In the presidential election of 2014, the final candidates agreed to a National Unity Government (22,23). Using this agreement, party members attempted to appoint their political allies to specific posts in the ministries. Our findings suggest that the official merit-based mechanism for the appointment of senior MoPH officials not followed, but that people were appointed based on political connections. This nepotism resulted in misuse internally by senior staff and externally by politicians.
Cultural issues, nepotism and conflicts of interest were highlighted in the MoPH ‘anti-corruption statement,’ (24). However, these issues were not mentioned in the ‘National Policy’ and ‘National Strategy’ (25). An ‘Anti-corruption strategy was endorsed by the MoPH (26), however, our findings suggest that this strategy was poorly implemented. Furthermore, anti-corruption strategies focused on the field/provinces/health system but not on central MoPH headquarters.
The socio-cultural and political influence consequences
In conflict-affected countries where there is nepotism and patronage networks, the ordinary population can be excluded from decision making and access to resources (27). In such societies corruption becomes the main problem as it reinforces the ethnicity, religion and class divisions with some groups enriching themselves at the expense of the country (28), resulting in economic and social instability (12). Our findings suggest that ethnicity or affiliation to ethnic political parties was a major factor in appointments, especially since employees unaffiliated to a political party were not supported to develop their career. This concurs with a report from South Africa where only people who were linked to the ruling political party, were provided with opportunities (29). Our study did not assess corruption directly; the findings represent our participants’ views. They explained that nepotism, favoritism and cronyism were everyday practice, which in their opinion, was corruption.
Afghanistan is not unique, nepotism and favoritism undermines authority and the public institutions in many settings (30,31). Smith found that although Nigerians were angry about corruption, they were also involved in it (32); whilst the majority agreed that corruption is wrong but when asked who is corrupt, their views were affected by their social ties, political advantage, and disadvantage (33).
The MoPH is not the only public ministry affected by political issues
People in our study reported that the MoPH is less affected by political issues than other ministries. A review by Giustozzi on the education of Afghanistan showed that politicians viewed schools as their source of patronage rather than a tool for ‘nation-building’ (34). This is similar to our findings that suggested the MoPH staff’s commitment was to their patron rather than to their country. Iraq is another conflict-affected country where ministries are driven by political factions racing for advantage or seeking to reward their supporters (35). The WHO reported that conflicts of interest and corruption affected the health system in countries such as Pakistan, Iraq, Jordan, Lebanon and Morocco (36). They explained that ensuring good governance and strengthening management systems for better transparency and accountability was a public health priority.
Leaders and Culture
MoPH staff were happy for the immediate benefits of nepotism and favouritism, but appeared unaware of the far reaching effects, the harm to the work environment, organization and how this undermines the whole health system. Schein suggests that leadership and organizational culture are two sides of the same coin in which leaders can influence the process of culture creation (37). Schein (37) describes the importance of leaders understanding their organizational culture.
“Culture is an abstraction, yet the forces that are created in social and organizational situations deriving from culture are powerful. If we don’t understand the operation of these forces, we become victim to them. Cultural forces are powerful because they operate outside of our awareness. We need to understand them not only because of their power but also because they help to explain many of our puzzling and frustrating experiences in social and organizational life.”
Our findings suggest that cultural issues distracted the MoPH, that it is the ‘victim’ of culture. The management of culture within an organization requires leadership and if a part of the culture is dysfunctional then it may be a reflection of the quality of leadership.
Although socio-cultural issues were part of daily life and both employees and directors knew they posed significant obstacles to organizational achievement, there was no report of strategies being implemented to eradicate such practices. Meanwhile, evidence suggests that directors were influenced by the socio-cultural practices, for instance, they were under pressure to give the employees good appraisal scores because of social relations rather than actual performance.
There is an urgent need to improve the management system, enforcing rules, in particular by making the hiring procedures transparent. Schein points out that if leaders instigate cultural evolution and change this will allow the group to survive in a changing environment (37). Leadership commitment, management skills and influence have the potential to transform poorly performing organizations into top performers (38).
Investment in training, specifically around socio-cultural issues, is needed to help leaders gain insight into their own behaviour. To support such an approach, Cumberland et al. (39) introduced a leadership competence development framework that develops self-awareness, where participants are given the opportunity to identify and reflect on their own values, attitudes and behaviour. Such training could also be supported by mentoring and coaching to raise participants’ self-awareness of their cultural biases.
As the first Afghan public ministry to investigate corruption and develop an anti-corruption strategy the MoPH showed courage and leadership. The enforcement of this strategy is unlikely to be easy and will have been delayed by current events. Ensuring that motivated and capable leaders are appointed on merit and that staff are treated consistently and fairly is an important goal for the future which will further strengthen the health system.
Study limitations and strengths
The first limitation is that the interview transcripts were in local language which prevented some team members from cross checking the data. However, a strength is that the coding process and the development of themes were all in English and were cross checked by the team. It is possible that there have been biases due to the survey and interview participants belonging to various political parties. A second strength is that none of the authors are members of a political party in Afghanistan, such membership could have affected this study.
As this research was conducted prior to the Taliban take over in 2021 the current situation will differ. Contemporary studies show that the health system is functioning but under threat facing many constraints such as the withdrawal of funding by some donors (40,41). For the moment ensuring funding from key donors is a priority so that essential services can continue, and further excess mortality and morbidity be avoided (42). The findings are, however, relevant to those working in similar contexts as they reveal the importance of exploring and understanding the impact of socio-cultural political issues on leaders and managers of health systems and other public institutions.
5. Recommendations
As the political and socio-cultural aspects were the main factors for low capacity in the MoPH and its performance, the current government should address this problem as soon as it is possible. This will help in making the solutions to other problems easier. The socio-cultural issues would be better identified in the policy and strategy of the MoPH and be placed high on the agenda to be solved with strict follow up. A disciplinary procedure for the people who commit behavior such as favoritism or nepotism would be helpful. If these issues are resolved, people will be prepared to focus and work towards national goals in the MoPH. It will help many other problems that were found in this study including consistency and fairness among staff members. This will also help competent people from diverse groups with different views to compete to enter the system, which will boost improvement.
Further research needs to assess the current extent and impact of socio-cultural and political issues on management capacity in the MoPH.
The MoPH would benefit from endorsing and implementing the anti-corruption strategy and monitoring progress as soon as it is feasible.
Initiating a training program to enable leaders and managers to reflect on their behavior and gain insights on their cultural biases might be very helpful for the MoPH and other ministries in Afghanistan.
Most of the health services in Afghanistan are supported by the non-governmental organizations. Therefore, it would be helpful for them to understand the complexity of the situation and be aware of the factors that affect the management capacity and the performance of employees.
Our findings suggest that the MoPH was less affected by political and socio-cultural issues than other ministries and that the MoPH had developed strategies to prevent the socio-cultural influences and corruption. Although it did not appear that these strategies had been fully implemented this was an important step that could be taken by other ministries - to recognize their problems and seek for the solutions.
Although every setting is unique, this study suggests that exploring the impact of socio-political issues on the functioning of health systems and those in leadership may be beneficial in understanding constraints to capacity and performance.
6. Conflict of interests
The authors declare that they have no conflict of interest.
7. References
- Feroz F. Health Gains in a Mix of Conflict and Development [Internet]. LSHTM; 2018 [cited 2021 Jan 7]. Available from: https://panopto.lshtm.ac.uk/Panopto/Pages/Viewer.aspx?id=cbc69ef1-0ae0-44ec-b887-d94a09be3325
- Roberts B, Guy S, Sondorp E, Lee-Jones L. A basic package of health services for post-conflict countries: implications for sexual and reproductive health services. Reproductive health matters. 2008 Jan 1;16(31):57-64.
- Najafizada SA, Labonté R, Bourgeault IL. Community health workers of Afghanistan: a qualitative study of a national program. Conflict and health. 2014 Dec;8(1):1-6.
- Ministry of Public Health (MoPH). National Health Policy 2015-2020. Kabul: MoPH; 2015.
- Newbrander W, Ickx P, Feroz F, Stanekzai H. Afghanistan's basic package of health services: its development and effects on rebuilding the health system. Global public health. 2014 Jul 21;9(sup1):S6-28.
- Turkmani S, Currie S, Mungia J, Assefi N, Rahmanzai AJ, Azfar P, Bartlett L. ‘Midwives are the backbone of our health system’: lessons from Afghanistan to guide expansion of midwifery in challenging settings. Midwifery. 2013 Oct 1;29(10):1166-72.
- WHO. Country Cooperation Strategy at a Glance. Kabul: WHO; 2018a.
- Lee JL. Afghanistan: A History from 1260 to the Present. Reaktion books; 2022 Mar 8.
- Ministry of Public Health (MoPH). A Basic Package of Health Services (BPHS) for Afghanistan. Kabul: MoPH; 2005.
- Ministry of Public Health (MoPH). National Health Policy 2015-2020. Kabul: MoPH; 2015.
- Giustozzi A, Ibrahimi N. Thirty years of conflict: drivers of anti-government mobilisation in Afghanistan, 1978-2011. Kabul: Afghanistan Research and Evaluation Unit; 2012 Jan.
- Eggerman M, Panter-Brick C. Suffering, hope, and entrapment: Resilience and cultural values in Afghanistan. Social science & medicine. 2010 Jul 1;71(1):71-83.
- Yin RK. Case study research and applications: Design and methods. 6th edition. Los Angeles: Sage; 2018.
- Robichaux C. Ethical competence in nursing practice: Competencies, skills, decision-making. Springer Publishing Company; 2016 Sep 7.
- Walliman N. Research methods: The basics. 2nd edition. New York City, NY: Routledge; 2018.
- Curtis E, Drennan J. Quantitative health research: issues and methods: issues and methods. McGraw-Hill Education (UK); 2013 Sep 1.
- Bryman A. Social research methods. Oxford university press; 2016.
- Gerrish K, Lathlean J. The research process in nursing. 7th edition. Oxford: Wiley Blackwell; 2015.
- Merriam SB, Tisdell EJ. Qualitative research: A guide to design and implementation. John Wiley & Sons; 2015 Aug 24.
- Braun V, Clarke V. Using thematic analysis in psychology. Qualitative research in psychology. 2006 Jan 1;3(2):77-101.
- Nepotism [Internet]. [cited 2021 Jan 11]. Available from: https://dictionary.cambridge.org/dictionary/english/nepotism
- John Kerry praises Abdullah and Ghani as Afghanistan’s struggles continue [Internet]. Guardian News and Media; 2014 [cited 2021 Jan 21]. Available from: https://www.theguardian.com/world/2014/sep/27/john-kerry-afghanistan-abdullah-ghani-power-money
- Afghan presidential rivals Sign Government Unity deal [Internet]. BBC; [cited 2021 Jan 21]. Available from: https://www.bbc.co.uk/news/av/world-asia-28712184
- Ministry of Public Health (MoPH). Statement: Addressing Corruption in the Health Sector. Kabul: MoPH; 2015b.
- Ministry of Public Health (MoPH). National Health Strategy 2016‒2020. Kabul: MoPH; 2016.
- Ministry of Public Health (MoPH). Anti-corruption Strategy 2017-2020: Laying the Foundations for Zero Tolerance of Corruption in the Health Sector. Kabul: MoPH; 2017.
- Imiera, PP. The corruption race in Africa: Nigeria versus South Africa, who cleans the mess first? De Jure Law J. 2020; 53:70-89.
- Goodson LP. Afghanistan’s endless war: State failure, Reginal polilitics, and the rise of the Taliban, Washington: University of Washington Press. 2001.
- ANC corruption is a major cause of South Africa’s failure – and the polls will show it | William Gumede [Internet]. Guardian News and Media; 2019 [cited 2020 Dec 14]. Available from: https://www.theguardian.com/commentisfree/2019/may/08/anc-corruption-south-africa-failure-polls
- Hampshire K. Pierce, Steven. Moral economies of corruption: state formation and political culture in Nigeria. xvi, 282 pp., maps, bibliogr. Durham, NC: Duke Univ. Press, 2016.£ 18.99.
- Harris D, Wales J, Jones H, Rana T, Chitrakar R. Human resources for health in Nepal: The politics of access in remote areas. London: Overseas Development Institute. 2013.
- Smith DJ. Corruption and “culture” in anthropology and in Nigeria. Current anthropology. 2018 Apr 1;59(S18):S83-91.
- Smith DJ. Moral Economies of Corruption: State Formation and Political Culture in Nigeria. Steven Pierce. Durham, NC: Duke University Press, 2016. 286 pp.
- Giustozzi A. Nation-building is Not for All. Kabul: Afghanistan Analyst Network. 2010.
- Looney RE. Reconstruction and peacebuilding under extreme adversity: The problem of pervasive corruption in Iraq. International Peacekeeping. 2008 Jun 1;15(3):424-40.
- BO I, HSPVQ B. WHO events addressing public health priorities. Eastern Mediterranean Health Journal. 2014:828.
- Schein EH. Organizational culture and leadership 4th Edition. San Francisco. 2010.
- Rendell N, Lokuge K, Rosewell A, Field E. Factors that influence data use to improve health service delivery in low-and middle-income countries. Global Health: Science and Practice. 2020 Sep 30;8(3):566-81.
- Cumberland DM, Herd A, Alagaraja M, Kerrick SA. Assessment and development of global leadership competencies in the workplace: A review of literature. Advances in Developing Human Resources. 2016 Aug;18(3):301-17.
- Andersen CT, Ayoya MA, Luo D, Samaha H, Shafique F, Chopra M. Afghanistan's health system is under duress, but has not collapsed. The Lancet. 2023 Feb 18;401(10376):554-5.
- Rubenstein L, Jalazai R, Spiegel P, Glass N. The crisis of maternal and child health in Afghanistan. The Lancet. 2023 Jan 14;401(10371):87-90.
- Safi N, Anwari P, Hemachandra N, Sidhu L, Ibrahimi AG, Rasekh A, Naseri S, Salemi W, Chikvaidze P. The need to sustain funding for Afghanistan health system to prevent excess morbidity and mortality. Eastern Mediterranean Health Journal. 2023;29(2):119-25.