- Available
- XML
- Download citation
- Statistics
- Share




Knowledge, and practice of women on breast cancer in Herat, Afghanistan: A cross-sectional study
show more
| Received 16 Jan 2023 |
Accepted 28 Apr 2023 |
Published 30 May 2023 |
Abstract
Background: Breast cancer prevalence is observed to be higher in developed economies, but the mortality rates due to the said disease tend to be similar or even higher among lower-income countries. Afghanistan is among these countries where breast cancer mortality has been predominant among the female population. This may be related late diagnosis and the presentation of the cancer at much later stages.
Methods: This cross-sectional study was conducted using a survey questionnaire administered from June 2021 to July 2021 among women living in Herat province of Afghanistan. It evaluated the participants’ knowledge and practice towards breast cancer. A total of 534 women answered the survey. Data was analyzed using IBM SPSS software.
Results: Lower level of knowledge about breast cancer and the limitations to the practice of breast self-examination (BSE) were found to be associated with such late detection and treatment. Using data collected in Herat Province of Afghanistan, this study examined the individual level sociodemographic factors related with the level of knowledge about breast cancer and also with the practice of BSE. It was found that 44% of the study sample of 534 women had high knowledge level. There were fewer still who performed BSE at about 12% of the respondents. Further examination showed that lower education attainment, albeit illiteracy, and the employment status were correlated with knowledge and practice surrounding breast cancer.
Conclusion: This entails the need to formulate programs targeting the specific needs of women with lower socioeconomic status to build capacity toward their health and wellbeing.
Keywords: Knowledge, Practice, Awareness, Breast Cancer, Herat-Afghanistan.
1. Introduction
Cancer, or neoplasms, is among the leading causes of mortality globally in recent years (1). In 2020, there were 18 million new cases of all cancers, excluding non-melanoma skin cancer, translating to a crude rate of about 232 cases per 100,000 persons (2). Five of the most common cases were breast, lung, colon and rectum, prostate, and non-melanoma skin cancer. In conjunction with being the most common new cancer cases, lung, colon and rectum, and breast cancer were found to be among the most common causes of cancer deaths as well. Breast cancer disproportionately affects women, with almost all new cases and deaths for this cancer type occurring in females (2).
The rate of breast cancer incidence in 2020 was higher in developed countries at almost 56 cases per 100,000 compared to about 30 per 100,000 cases in developing countries (3). The higher rate of breast cancer in developed countries, such as those in Western Europe and North America, has been attributed to differences in reproductive, nutritional, and hormonal factors, but also, mammographic screening has been more prevalent (4,5). Global regions with the lowest prevalence rates, at less than 40 cases per 100,000 population, were Central America, Eastern and Middle Africa, and South Central Asia (3). Despite the observation that incidence rates have been increasing in developing countries (4), the mortality rate of breast cancer for the said countries were comparable or even higher than higher-income countries (3).
Breast cancer mortality rates were noted to be higher in many lower-income countries than others that may be attributable to its presentation at later stages of the disease. The World Health Organization (WHO) indicated that, although population-based mammography screening is optimal for addressing this healthcare challenge, it may not be feasible for lower-income countries (6). Breast cancer awareness and early detection are emphasized in these settings (7). Having knowledge of the disease's symptoms and access to proper medical care has been shown to be effective in late-stage presentation of breast cancer (7–9). Breast self-examination (BSE) is an important measure to know and perform in lower economic capacity settings (10) but, it is also in these contexts where such knowledge bears shortcomings (11,12).
This study focused on the knowledge and practice of Afghan women with regard to breast cancer. There were 22,817 new cases of cancer of any type in 2020 in Afghanistan. About 13.9% of these new cases were breast cancer. When disaggregated by gender, new cases that were female amounted to 12,289 or about 54% of the total new national cases. A quarter (25.8%) of these new cancer cases among women were of the breasts. The previously mentioned figures were morbidity cases. In terms of mortality, 11.1% of the total deaths due to cancer was attributed to breast cancer. It was noted that diagnostic and therapeutic infrastructure and medical personnel have been lacking in the country resulting to delayed diagnoses and insufficient treatment (13). It was also suggested that, if Afghanistan’s case were to be compared with other lower-income societies, awareness level may also be low but, this has yet to be measured concretely in the individual level in communities. As such, the present study aimed to collect and observe data regarding the knowledge and practices of adult women with regards to breast self-examination and breast cancer in the western region of Afghanistan – the Herat province.
2. Materials and Methods
Data
The survey design and questionnaire used in this study were obtained from the research of Okobia and colleagues (14), and we obtained their permission to use it in our study. This questionnaire-based, cross-sectional study was conducted from June 2021 to July 2021 among women aged at least 18 years old living in Herat province of Afghanistan. The simple random sampling method was used to collect data for this study. To determine the target sample size of participants, the formula N = Zα2P(1−P)/d2 was used, with α set at 0.05 and Zα set at 1.96. The acceptable margin of error for proportion, d, was estimated at 5%. Ethical approval for the conduct of this study was obtained from the Center for Epidemiological Studies [ACES] Ethical Committee bearing the reference number (#21.0023).
The questionnaire was translated to the Dari language. Being the lingua franca of the province, the prospective respondents were to be limited to speakers of the Dari language. A pilot study was conducted among thirty female participants. After the necessary changes to adapt the said questionnaire in the local context, the final survey instrument consisted of twenty-four items divided into three information groups: the socio-demographic, knowledge and attitude, and the breast examination practice.
Data was collected by medical member of the Afghanistan Medical Students Association (AMSA) in Herat province of Afghanistan. These data enumerators were trained on how to select participants, demonstrate the study goal how to ask the questions, and finally take a consent letter from the participant.
Measures
Respondents were asked for individual characteristics in the survey as mentioned above. For the present study, sociodemographic information regarding age, education, marital status, urban-rural residence, and occupation. In the following group information domain, knowledge and attitude about breast cancer were utilized. Each item had three options as follows: “Yes”, “No”, and “Do not know”. The final response option of ‘Do not know’ was retained in the univariate distribution to accurately show the level of knowledge of the participating individuals. For the subsequent bivariate analyses, a threshold was set in order to determine who among the participants had a good level of knowledge about breast cancer. This threshold was responding correctly to more than seven out of the thirteen questions for this information domain. In the final information group in the survey, the practice and clinical breast examination consisted of six items.
Analysis
The characteristics distribution of the sample was observed primarily. Next, the response distribution to breast cancer awareness and the practice of breast examination were also viewed. Upon categorizing the sample’s level of knowledge of breast cancer and their adherence to the practice of clinical and self-examination, the chi-square [χ2] test was performed between the aforementioned indices of knowledge and practice and the sociodemographic variables. The alpha level of statistical significance was set at 95%.
3. Results
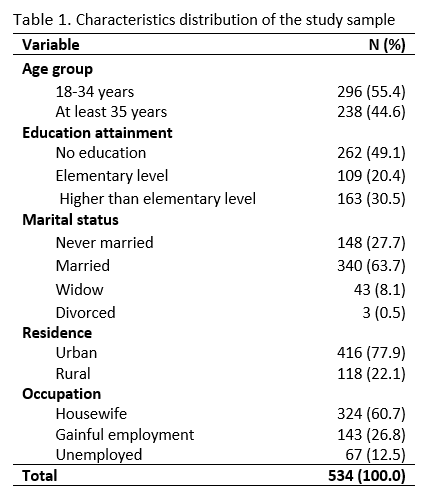
A total of 534 women participated in this study with the age range of 18 to 68 years. The mean age of the study sample was 34.58 (Table 1). More than half (55.4%) of the respondents were in the age group of 18 to 34 years old. Many of the them have no education and about 31% have higher than elementary level of schooling. Most of the women were married (63.7%), lived in an urban area (77.9%), and were housewives (60.7%).
Almost 70% of the individuals in the sample were aware that breast cancer is the most common cancer among women (Table 2). The majority also had the thought that such cancer could be experienced more by older people (73.4%) and that the predisposition of having it is hereditary (63.5%). Most also answered positively regarding the curability of breast cancer and the importance of early diagnosis for improved outcome of treatment. On the other hand, there were a few (14.6%) who believed that such disease was caused by evil.

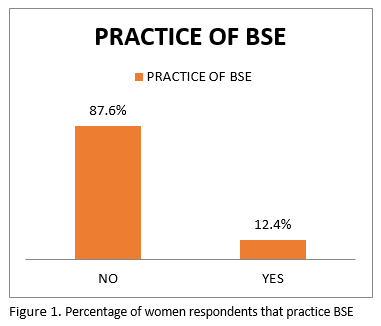
In Table 3, practices surrounding breast examination are presented. It was observed that about 88% of those in the sample practiced BSE. As shown in Figure 1, Between those who do practice self-examination, the frequencies of self-checking vary much from doing it once a month (3.9%) to those doing it once or twice a year (0.2%).


As shown in Figure 2, Many of the women’s primary source of knowledge about BSE were from their personal network consisting of family and friends and the common cause of not doing the practice was the perception that they do not have any problem with their breasts. In the case of CBE, there were fewer of those in the sample who practice it (4.9%). Most of the women also had the self-perception of good breast health that is why they do not engage in CBE.
Table 4 shows the bivariate distribution of the score categories of the respondents whether they have a low or high level of knowledge about breast cancer. Regardless of age, it was observed that fewer women had a high level of knowledge. Given this, age groups along with marital status and residence were observed to lack association with knowledge scores. Women with higher than elementary level of schooling and those with gainful employment or were unemployed had been found to have higher scores than their counterparts in respective categories.

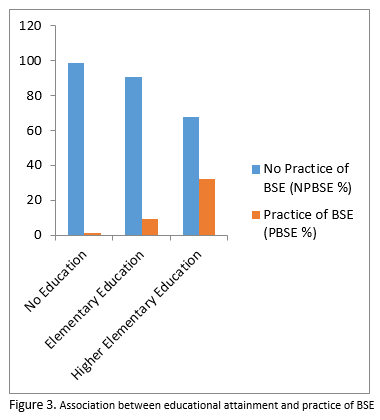
The association of individual characteristics and the practice of BSE are in Table 5. It was found that based on this sample, age and marital status lacked statistical significance between the association of sociodemographic factors and the practice of BSE. As shown in Figure 3, Having high level of knowledge and better educational attainment were observed to have better adherence to self-examination. On the other hand, residing in a rural area and being a housewife were seen to be among those who do not practice BSE.
4. Discussion
The findings in this study based on a sample of female adults in Herat in Afghanistan showed that the level of knowledge about breast cancer needs further improvement. It was also observed that women, including those who possess adequate knowledge of the said disease, need to be encouraged to perform clinical or self-examination of the breast due to the low prevalence of the practices. These observations confirm the contention that lack of awareness of breast cancer contribute to late diagnoses and therefore increases the probability of mortality among the population (13).
As observed in the present study, a large majority of women do not practice BSE regardless of residence but was suggested the figure of non-practice in rural areas was more pronounced. This is a precarious situation because in societies where clinical screenings are in need of much advancement, such as in Afghanistan (13), self-examination and self-detection can be the more prevalent method of treating breast cancer in earlier stages as observed in rural Peru (15). In the national health strategy of Afghanistan that was set from 2016 to 2020, the need for developing control for chronic diseases was underscored (16) but, there was no concrete and actionable measures specified because of the low number of medical personnel and proper infrastructures. This situation presents a disadvantage for women especially in the rural areas to be better informed about breast cancer. On the other hand, the shortcomings in the national level also emphasizes the need for community-level actions to develop the capacity of the population about their health.
The socioeconomic background of women was observed in this study to be consistently associated with having a higher level of knowledge on breast cancer and practice of BSE. Such findings are in lieu of other studies such as those in different countries in Africa (9,12,17). The low level of knowledge and non-practice of breast examinations reflect the social and health disparities women experience when they have low education attainment or even illiterate and when they are engaged in unskilled work. Human capital development, which subsumes education and employment, has been shown to have positive effects on health (18). In this regard, building the capacity of women on how they view themselves is a key driver toward minimizing disparities in breast cancer disparities in low- and middle- income countries (LMICs) (9,19, 20).
The level of awareness among women in the study sample were shown to be associated with educational attainment. This suggests that overall development in the education of women needs to come to fruition in the longer term (21). What is needed in the short term are targeted programs that addresses the needs and capacity of women in the Herat province. These actions can include information drives and community education initiatives which are guided by the background of the female population that may be illiterate and have lower socioeconomic status. Such activities have to be tailored in order to prevent being disruptive of women’s duties whether they are housewives or engaged in gainful employment.
The present study has shown the need for an understanding of the knowledge and practices of women in the community level as in districts of Herat province. There are limitations that need to be presented. Firstly, this was a cross-sectional study and therefore no causation can be established. Also, the sample included adult women in Herat but was limited to those who can communicate in the Dari language. Women in the health sector including volunteers were also excluded as they may affect the outcome of the survey results due to their training background. For future studies, the modest sample size used in the present study can be increased and the survey may be performed in more provinces in order to establish comparisons in the experience of women and breast health.
5. Conclusion
The observations here have shown there is space for development surrounding knowledge and practices about breast cancer. The study sample have demonstrated low level of awareness in general and that the prevalence of breast self-examination was low as well even when women have sufficient knowledge about the chronic disease. What underscores these aspects of shortcomings in health information and practices is the disparities in education and employment among women. The need to educate them and establish the importance of self-diagnosis and attending proper medical facilities for treatment and care should be formulated according to the background of individuals.
6. Ethics approval and consent to participate
Ethical approval for the conduct of this study was obtained from the Afghanistan Center for Epidemiological Studies [ACES] Ethical Committee bearing the reference number (#21.0023). During the initial contact with the participants, a description of the study was presented to them. Informed consent or verbal approval was obtained from all the participants of this study. All methods were carried out in accordance with relevant guidelines and regulations.
7. Consent for publication
Not applicable.
8. Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
9. Competing interests
The authors declare that they have no competing interest.
10. Funding
No external funding was received for this study.
11. Authors' contribution
F.B designed the study. M.Y., A.R., and E.N. contributed in data collection of this study. F.B. analyzed the data. F.B., G.O., Y.E., and M.V. prepared the draft of the manuscript. F.A.S., and D.E.L.P. finalized the manuscript. All authors reviewed the manuscript.
12. Acknowledgements
We would like to thank the Center for Epidemiological Studies of Afghanistan for their guidance and help with this study.
13. References
- World Health Organization. Cancer [Internet]. 2022 [cited 2022 Apr 16]. Available from: https://www.who.int/news-room/fact-sheets/detail/cancer
- International Agency for Research on Cancer. Cancer Today [Internet]. 2020 [cited 2022 Apr 16]. Available from: https://gco.iarc.fr/today/home
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71[3]:209–49.
- Bray F, McCarron P, Parkin DM. The changing global patterns of female breast cancer incidence and mortality. Breast Cancer Res. 2004;6[6]:229–39.
- Breen N, Gentleman JF, Schiller JS. Update on mammography trends: Comparisons of rates in 2000, 2005, and 2008. Cancer. 2011;117[10]:2209–18.
- World Health Organization. WHO position paper on mammography screening [Internet]. 2014 [cited 2022 Apr 16]. Available from: https://www.who.int/publications-detail-redirect/who-position-paper-on-mammography-screening
- Birnbaum JK, Duggan C, Anderson BO, Etzioni R. Early detection and treatment strategies for breast cancer in low-income and upper middle-income countries: a modelling study. Lancet Glob Heal. 2018;6[8]:e885–93.
- McCormack V, McKenzie F, Foerster M, Zietsman A, Galukande M, Adisa C, et al. Breast cancer survival and survival gap apportionment in sub-Saharan Africa [ABC-DO]: A prospective cohort study. Lancet Glob Heal. 2020;8[9]:e1203–12.
- McKenzie F, Zietsman A, Galukande M, Anele A, Adisa C, Parham G, et al. Drivers of advanced stage at breast cancer diagnosis in the multicountry African breast cancer – disparities in outcomes [ABC-DO] study. Int J Cancer. 2018 Apr 15;142[8]:1568–79.
- International Agency for Research on Cancer. Breast self-Examination [BSE] [Internet]. 2022 [cited 2022 Apr 18]. Available from: https://screening.iarc.fr/breastselfexamination.php
- Alsaraireh A, Darawad MW. Breast cancer awareness, attitude and practices among female university students: A descriptive study from Jordan. Heal Care Women Int . 2017;39[5]:571–83.
- Dadzi R, Adam A. Assessment of knowledge and practice of breast self-examination among reproductive age women in Akatsi South district of Volta region of Ghana. PLoS One. 2019;14[12]:e0226925.
- Niazi A-R, Jami AA, Shams AZ, Mahmoodi AS, Krapfl E, Falk S, et al. Establishing a breast cancer center in Herat, Afghanistan: An implementation study. Glob Heal J. 2021;5[4]:204–8.
- Okobia MN, Bunker CH, Okonofua FE, Osime U. Knowledge, attitude and practice of Nigerian women towards breast cancer: A cross-sectional study. World J Surg Oncol. 2006;4[1]:1–9.
- Romanoff A, Constant TH, Johnson KM, Guadiamos MC, Vega AMB, Zunt J, et al. Association of previous clinical breast examination with reduced delays and earlier-stage breast cancer diagnosis among women in Peru. JAMA Oncol. 2017;3[11]:1563–7.
- Ministry of Public Health. National Health Strategy 2016‒2020 Sustaining Progress and Building for Tomorrow and Beyond | Global database on the Implementation of Nutrition Action [GINA] [Internet]. Kabul; 2016 Sep [cited 2022 Apr 17]. Available from: https://extranet.who.int/nutrition/gina/en/node/25727
- Pace LE, Mpunga T, Hategekimana V, Dusengimana J-MV, Habineza H, Bigirimana JB, et al. Delays in breast cancer presentation and diagnosis at two rural cancer referral centers in Rwanda. Oncologist. 2015;20[7]:780–8.
- Lutz W, KC S. Global human capital: Integrating education and population. Science [80- ]. 2011;333:587–92.
- Ginsburg OM. Breast and cervical cancer control in low and middle-income countries: Human rights meet sound health policy. J Cancer Policy. 2013;1[3–4]:e35–41.
- Okaliwe G, Nja GME, Ogunkola IO, Ejemot-Nwadiaro RI and Lucero-Prisno DE III (2021) Breast Cancer Knowledge and Mammography Uptake among Women Aged 40 Years and Above in Calabar Municipality, Nigeria. Asian Journal of Medicine and Health. 19(8): 1-10. DOI: 10.9734/ajmah/2021/v19i830351
- Ngoma T, Mandeli J, Holland JF. Downstaging cancer in rural Africa. Int J Cancer. 2015;136[12]:2875–9.